Humacyte makes "spare parts for people" and will hear from the Food and Drug Administration soon about whether those parts will be approved to treat patients.
Humacyte is a biotech company in Durham, NC, that makes artificial blood vessels. The Artificial Tissue Engineered Vessels or ATEVs have been in development for almost two decades, but so far have been available only to patients in clinical trials. But with an FDA decision coming up, that could change. And an approval would be a win not only for the company, but also for the growing research and development presence in the Triangle region.
Bringing an innovative product to the market
Humacyte's ATEVs have been tested extensively in clinical trials for more than a decade, and have been in development since 2005. Humacyte's CEO and co-founder Laura Niklason is hopeful that after many years of work, the FDA will approve the ATEVs for use on August 10.
"That will allow us to launch our product into hospitals where trauma surgeons and vascular surgeons will be able to use it to treat patients who are wounded," she said.
Those could be patients who have been in car accidents or suffered gunshot wounds, and receiving an artificial blood vessel could salvage limbs or even save lives.
"Our engineered tissues, when we implant them, they don't have any cells in them," Niklason said. "But after they do get implanted, cells from the patient sort of crawl in and take up residence in the tissue and turn it into a living tissue. It becomes self."
Scientists have dreamed about this kind of engineered tissue for decades, but so far Humacyte is the only company that has been able to make a product like that a reality.
"It's very exciting for the company, because this represents an incredibly long journey," Niklason said. "To get to this point where we're getting to approval for something that's really fundamentally new is pretty cool."
Blue Cross and Blue Shield of North Carolina (Blue Cross NC) launched the first phase of a statewide, transformational commitment to improving youth mental well-being, resiliency and connectivity. The initial phase begins with comprehensive enhancements to the company’s mental health offerings, targeting improvements in support services and access to care across all 100 North Carolina counties.
This foundational step is the beginning of an ongoing, multi-year effort that comes in response to insights gained from the Extra Miles Tour, a statewide listening tour completed in 2023. Throughout the tour, company leaders heard firsthand about widespread feelings of lacking purpose, social isolation and loneliness among young North Carolinians – underscoring the pressing and urgent need to improve the well-being and connectivity of youth across the state. Community leaders are stepping in to fill the gaps, but more work is needed to accelerate and elevate their work.
Medscape is making available their annual Physician Compensation Survey. Over 100,000 physicians contributed, providing comprehensive salary information from across the United States. This interactive format makes it easy to compare salaries by specialty, practice setting, and location.
Behind the data
Only full-time (non-resident) salaries are included in our data set.
For employed physicians, base salary, bonus, and profit-sharing contributions are included.
For owners and partners, income is earnings after taxes and deductible business expenses before income taxes.
All data is aggregated geographically to the nearest DMA (Designated Market Area) to ensure physician anonymity.
Please share your stories here on how corporate interventions in medicine have impacted you and your practice. This includes private equity acquisitions, noncompete agreements, management service organizations, and any business intervention that has impacted your ability to practice medicine.
NCMS member Dr. John Catanzaro awarded Dr. John “Jack” Rose Distinguished Professorship, launches new Electrophysiology Fellowship at ECU Health
Dr. John Catanzaro, professor and chief of the Division of Cardiology at the Brody School of Medicine at East Carolina University and director of the East Carolina Heart Institute at ECU Health Medical Center, was recently honored with the prestigious Dr. John “Jack” Rose Distinguished Professorship, recognizing his significant contributions to improving health care delivery, excellence in clinical medicine, administration and academic advancement, including formation of the first Clinical Cardiac Electrophysiology Fellowship at ECU Health.
The Rose Professorship, established by ECU Health and East Carolina University through the ECU Health Foundation and state funds, honors Dr. Rose, a renowned cardiologist and professor. This endowed title supports the director of the East Carolina Heart Institute recognizes Dr. Rose’s exceptional contributions to cardiology and medical humanitarian work. Dr. Rose, who joined ECU Health in 1982 and the Brody School of Medicine in 1990, is celebrated for his dedication to patient care, teaching, and community service. Recipients of this professorship are expected to embody his ideals and passion for teaching, inspiring future generations of medical professionals.
Read the full article on this prestigious honor here.
Duke Health is notifying patients that their coverage could be impacted by a contract dispute with UnitedHealthcare, one of the U.S.'s largest insurers.
Why it matters: If a deal isn't reached by Oct. 31, Duke Health patients with UnitedHealthcare insurance will be considered out of network, meaning most will need to pay more out of pocket or find a new doctor or health system, Duke informed patients in a Monday letter obtained by Axios.
Around 170,000 Duke Health patients throughout the state could be affected if the UnitedHealthcare contract expires, per Duke Health.
The big picture: This isn't the first time a health system in the Triangle has gone public with its contract negotiations with UnitedHealthcare.
Last year, UNC Health warned patients of potential disruption due to contract negotiations with the insurer but ultimately came to an agreement four days before its contract expired.
Zoom in: Duke and UnitedHealthcare have been negotiating since April, according to a UnitedHealthcare spokesperson, and the insurance company sent its fourth proposal to Duke on Tuesday.
What they're saying: Duke Health said in a statement to Axios that it hopes UnitedHealthcare will agree to a new contract that fairly reimburses Duke.
In its letter, Duke Health said UnitedHealthcare's reimbursements have not kept up with inflation.
"To continue serving the patients and families who trust us for unmatched quality, expertise and the best possible outcomes, we must ensure that UnitedHealthcare — and all insurance companies we partner with — reimburse Duke Health at fair rates that cover the rising cost of care," the health system said in the statement. "That is why we are negotiating today."
The other side: The UnitedHealthcare spokesperson said its priority is reaching an agreement with Duke Health.
"We delivered a new proposal on Aug. 20 that includes meaningful rate increases that would ensure Duke continues to be reimbursed similar to peer health systems," UnitedHealthcare spokesperson Cole Manbeck said in a statement.
"We will remain at the negotiating table as long as it takes to reach an agreement," Manbeck added. "We hope Duke joins us there and works toward a solution that North Carolina families and employers can afford."
A three-year study of tirzepatide – a medication approved in the US as Mounjaro for diabetes and Zepbound for weight loss – found that when adults who had prediabetes and obesity or overweight used it weekly, it lowered their risk of progression to diabetes by 94% compared with a placebo, according to drugmaker Eli Lilly.
The company said Tuesday that people who got a 15-milligram (mg) dose of the medicine also had an average decrease in body weight of nearly 23%, compared with 2.1% in those who got a placebo.
During a 17-week off-treatment follow-up period, people who had stopped using tirzepatide began to regain weight, Lilly said in a news release, and there was “some increase in the progression to type 2 diabetes.”
“The most frequently reported adverse events were typically gastrointestinal-related and generally mild to moderate in severity,” Lilly said. “The most common gastrointestinal-related adverse events for patients treated with tirzepatide were diarrhea, nausea, constipation and vomiting.”
Prediabetes is a condition in which blood sugar, or glucose, levels are higher than normal but don’t reach the criteria for a diagnosis of diabetes. It affects about 1 in 3 adults in the US – 84 million people – and about 70% will go on to be diagnosed with diabetes. Lifestyle changes – especially weight loss – have generally been considered the most important management tool.
Tirzepatide works by mimicking hormones that stimulate the release of insulin, increase feelings of fullness and reduce appetite. It targets two hormone receptors, GIP and GLP-1. It’s part of a new class of drugs that includes semaglutide, known as Ozempic for diabetes and Wegovy for weight loss, which have skyrocketed in popularity in recent years.
In earlier trials of tirzepatide, the medication was found to yield more average weight loss than other approved medicines, and in November, the US Food and Drug Administration approved it for people with obesity or those characterized as overweight with at least one weight-related health condition, such as high blood pressure or heart disease. Like similar drugs, it’s used as a shot patients give themselves once a week and is recommended on top of a reduced-calorie diet and increased exercise.
The results of the new trial “will be submitted to a peer-reviewed journal and presented at ObesityWeek 2024” in November, Lilly says. [source]
Scientists have found that human beings age at a molecular level in two accelerated bursts – first at the age of 44, and then again at 60.
In a study published in the journal Nature Aging, scientists at Stanford University and Nanyang Technological University in Singapore followed 108 participants over several years to observe aging changes in their molecules — RNA, proteins and participants’ microbiomes.
The scientists found that human aging does not happen in a gradual, linear way. Rather, the majority of the molecules they studied showed accelerated, non-linear changes at the ages of 44 and 60.
Xiaotao Shen, an assistant professor in microbiome medicine at Nanyang Technological University and first author of the study, told CNN that the results show “we are not becoming old gradually.” Some points in time are particularly important for our aging and health, he added.
For example, the ability to metabolize caffeine notably decreases – first around the age of 40 and once more around 60. Components involved in metabolizing alcohol also diminish, particularly around the age of 40, Michael Snyder, chair of the department of genetics at Stanford and an author of the study, told CNN, referring to the two waves of aging.
Pharmaceutical group GSK has been granted breakthrough therapy designation by the US Food and Drug Administration (FDA) for a key lung cancer treatment.
The breakthrough therapy designation is designed to expedite the development and review of drugs with the potential to treat a serious condition.
Only treatments that are shown to offer a substantial improvement over currently available therapy are awarded this designation.
GSK’s treatment, its investigational B7-H3-targeted antibody drug conjugate, or GSK’227, is being evaluated for the treatment of patients with extensive-stage small-cell lung cancer.
The drug is aimed at patients who have seen disease progression on or after platinum-based chemotherapy.
The FDA breakthrough therapy designation has been awarded based on data from the drug’s ongoing phase one trial of more than 200 patients.
The trial’s results will be presented at the 2024 World Conference on Lung Cancer at the beginning of September.
Lung cancer is one of the most common cancers worldwide, and in the US, approximately 15 per cent of all lung cancers are small-cell.
What’s more, of those patients with small-cell lung cancer, 70 per cent have extensive-stage disease, according to GSK. That means the cancer has spread to one or both lungs and/or other parts of the body.
The five-year survival rate for these cancers is three per cent.
GSK acquired exclusive worldwide rights, excluding China’s mainland, Hong Kong, Macau, and Taiwan, from Hansoh Pharma earlier this year to progress the clinical development and commercialization of GSK’227.
Hesham Abdullah, senior vice president, global head oncology, research and development, GSK, said: “Extensive-stage small-cell lung cancer is aggressive with poor prognosis and significant need for new treatments. Today’s breakthrough therapy designation supports our ambition to accelerate GSK’227 for these patients as part of our broader antibody drug conjugate program focused on developing new treatment options with transformational and first-to-market potential.” [source]
HHS (through FDA, NIH, and others) is collecting data on medications you are trying for your patients’ Long COVID symptoms.
Their seeking to learn whether you feel any of these medications have improved your patients’ symptoms, have had no impact, or have made your patients’ symptoms worse.
Share your experience through the CURE ID mobile app or visit the CURE ID website.
In addition, you can explore treatment data such as case reports, clinical trials and more.
Buprenorphine Initiation and Linkage to Outpatient Services: Navigating Complex Care for Patients with Opioid Use Disorder in the Emergency Department Setting
Thursday, Aug. 22
2:30-4:00pm ET
This is a 90-minute training to discuss the pathophysiology of substance use, with a focus on navigating complex care for patients with OUD in the emergency department setting. This presentation will focus primarily on educating ER providers on the current climate of substance use in WNC and the best tactics and techniques to care for incoming patients and linking them to outpatient services.
Objectives
Describe complex care for patients with OUD in the emergency department
Foster confidence and comfort with tactics and techniques for linking incoming patients to outpatient services
Discuss how to support & educate patients to apply harm-reduction management techniques in the ED setting and linking to care quickly and appropriately
The North Carolina Department of Health and Human Services announced Blue Cross Blue Shield NCwas selected to operate the Children and Families Specialty Plan. A first-of-its-kind initiative, the CFSP is a single, statewide NC Medicaid Managed Care plan that will wrap Medicaid-enrolled children, youth and their families in the child welfare system with seamless, integrated and coordinated health care.
Supporting children served by the child welfare system requires a close coordination across multiple systems and partners to ensure we support preserving families, reunification and securing permanency to ensure the best outcomes. Children and families in the child welfare system often find it hard to navigate getting the health care, social services and mental health care they need. The CFSP is designed to support this population by providing health care and mental health care coverage that follows the person — regardless of their geographic location or situation — and works across all these multiple systems.
"This plan will ensure there is a unified system of care and clear accountability when it comes to improving the health and wellbeing of our kids living with the most complex challenges," said NC Health and Human Services Secretary Kody H. Kinsley. "We continue to improve how we serve people, so it’s more efficient and promotes better outcomes."
The CFSP provides comprehensive coverage for all services provided by the Standard Plan in addition to most Tailored Plan services, such as 1915(i) Home and Community-Based Services and enhanced behavioral health and residential services. It also includes a broad range of behavioral health services such as outpatient therapy, inpatient treatment, and crisis and therapeutic residential options for children. Additionally, the CFSP is responsible for addressing unmet health-related resource needs, including housing, food, transportation, and interpersonal violence. The plan also covers pharmacy, long term services and supports (LTSS) and Intellectual/ Developmental Disability (I/DD) services.
At launch, the CFSP will operate statewide, offering robust care management to approximately 31,000 current and former foster care children and youth that will be enrolled automatically. Children of these eligible populations will also be automatically enrolled at launch and maintain enrollment while their parents are enrolled. In line with the plan’s goal to support and strengthen families, the plan will also be available to parents and family members of children and youth served by the child welfare system, including those receiving Child Protective Services (CPS) In-Home Services. NCDHHS is currently working on estimating this population size, and service to family members will be available no sooner than July 2026.
"As we put this plan into action the department recognizes the importance of implementing a whole-person centered, well-coordinated system of care that will support Medicaid-enrolled children, youth and families served by the child welfare system," said Deputy Secretary of NC Medicaid Jay Ludlam.
Since 2021, NCDHHS has been leveraging the move to managed care for NC Medicaid to build an innovative health care delivery system that puts the health of beneficiaries at the forefront. Under Medicaid Managed Care, NC Medicaid Standard Plans and the Eastern Band of Cherokee Indians Tribal Option launched on July 1, 2021, followed by Behavioral Health I/DD Tailored Plans on July 1, 2024.
More information about the transition to NC Medicaid Managed Care can be found on the Medicaid website at medicaid.ncdhhs.gov/transformation.
The first CFSP contract was awarded to Blue Cross Blue Shield NC after a competitive selection process, and the term will last four years. Only entities operating as NC Medicaid Standard Plans, NC Medicaid Behavioral Health I/DD Tailored Plans and any other entity that meets the definition of a Prepaid Health Plan under NCGS § 58-93-5 or the 2023 Appropriations Act were able to bid on the contract.
Three grant opportunities totaling $4.5 million will support local partners in developing community-based initiatives to improve equitable access to mental health services, expand peer support services and strengthen family and caregiver support services, says North Carolina Department of Health and Human Services.
"Behavioral health is essential to health and these investments build on the near $1 billion we’re investing to improve the mental health system of care in North Carolina," said NC Health and Human Services Secretary Kody H. Kinsley. "These grant opportunities will help close health disparities by focusing on the unique needs of marginalized communities and empowering those with lived experience to be key to the solution."
NCDHHS will award Mental Health Block Grant funds to community-based partners to build or expand mental health services and supports for North Carolinians, including those with substance use and/or intellectual and developmental disabilities.
Specifically, the grants will be used to implement:
Community-Based Mental Health Initiatives: Projects that expand access to mental health supports for the LGBTQIA+ community, faith-based communities, people over the age of 65 and non-native English speakers, who often encounter unique challenges to finding and accessing culturally competent care. Projects should address barriers to care, promote culturally competent and trauma-informed services and foster resilience among these communities.
Peer Services: Peer Respite and Peer Living Room Models that serve as community-based alternatives to emergency departments or hospitals for crisis and recovery services. These programs provide peer-supported crisis, mental health and substance use recovery services. Programs will be administered by Certified Peer Support Specialists, who provide trauma-informed services supported by their lived experiences navigating the mental health system.
Family and Caregiver Support Services: Programs that offer support for family members who are caregivers and siblings of loved ones requiring intensive care for behavioral health, substance use, intellectual or developmental disabilities, traumatic brain injury or co-occurring conditions. Services provide an essential support and advocacy for family caregivers while ensuring continuity of care for their loved one.
Eligible organizations who would like to partner with NCDHHS in developing mental health solutions in their communities are encouraged to submit a proposal or application for funding through the Mental Health Block Grant. To learn more, visit the DMHDDSUS grant opportunities page.
"These grants are part of our ongoing work to improve how North Carolinians access mental health and well-being services both for themselves and for the people they love," said Kelly Crosbie, MSW, LCSW, Director of the NCDHHS Division of Mental Health, Developmental Disabilities, and Substance Use Services. "We are committed to fostering a system of equitable, compassionate, whole-person care that can move families and communities from a state of crisis into long-term recovery."
Investing in community-based services supports NCDHHS’ goal to ensure every North Carolinian has access to the right care, in the right place, at the right time to meet their mental health needs. The department is investing a historic $835 million to transform behavioral health services and build a system where everyone has someone to contact, someone to respond and a safe place for care whenever they need it.
The Centers for Medicare & Medicaid Services (CMS) Center for Medicare and Medication Innovation (“Innovation Center”) announced the 2024 Rural Health Hackathon – a series of in-person, collaborative sessions designed to generate and construct creative and actionable ideas to address rural health challenges.
The 2024 Hackathon builds on CMS’ extensive outreach to rural communities through site visits and listening sessions to better understand rural health care issues. Through these solution-oriented events, the CMS Innovation Center will bring together rural health community care providers, community organizations, industry and tech entrepreneurs, funders, policy experts, and beneficiaries to leverage the wisdom and experience of the crowd.
Hackathon attendees will generate new ideas to address some of the top challenges impacting health care in rural health settings and drive action to improve clinical outcomes, increase access, and better care experience for both patients and providers in rural communities.
Interested parties have two ways to participate:
In-Person Hackathon: Engage with other dedicated experts to solve some of the toughest challenges facing rural communities through one of the in-person convenings hosted in three cities this summer:
Wilson, North Carolina: August 29, 2024Please note that there is no virtual option for these events due to their collaborative, hands-on structure.
Virtual Idea Submission: Submit your written concepts to address top rural health challenges using this form. All concepts must be submitted no later than September 9, 2024, at 11:59PM EST. Please note that late submissions will not be considered.
Top ideas with greatest opportunity for action will be highlighted in a public CMS Innovation Center report and connected with leading health policymakers and potential private or non-profit partners in the field. See below for details on how to participate.
August is National Immunization Awareness Month (NIAM), a time to highlight the importance of vaccination for people of all ages. CDC recently published reports on the benefits of vaccination and updated guidance:
CDC’s Advisory Committee on Immunization Practices updated their recommendations for the use of respiratory syncytial virus (RSV) vaccines in adults who are 60 or older. See CDC's report.
Researchers concluded that routine childhood immunizations have been an important cost-saving public health strategy. Read theCDC report.
All staff in healthcare practices, including non-clinical staff, play important roles during NIAM:
Join HRSA’s National Minority Donor Awareness Month webinar. Speakers will discuss how to address cultural barriers and share effective donation outreach strategies. Hear from experts and personal stories that highlight the impact of donation and transplantation.
Live translation will be available in Spanish and English.
As North Carolinians navigate through another hurricane season, officials with the North Carolina Emergency Management and the Department of Health and Human Services warns against use of gasoline-powered generators, outdoor grills and camp stoves in enclosed spaces.
Carbon monoxide is an odorless, colorless gas produced whenever fuel is burned. In an enclosed space, such as a home, garage, car or camper, carbon monoxide can build up to deadly levels quickly. Even low levels of carbon monoxide can cause dizziness, fatigue, nausea, headaches, confusion or fainting. If you are experiencing these symptoms, get to fresh air immediately and seek medical attention.
High levels of carbon monoxide can be deadly within minutes. Carbon monoxide poisoning can be fatal to anyone, especially children, pregnant women, older adults and those with chronic illness. People who are sleeping or intoxicated can die from carbon monoxide poisoning without ever becoming aware of their symptoms.
Proper safety precautions should be used by anyone testing or using a generator or other fuel burning device during storms. These precautions include the following:
Do not use gasoline-powered tools or engines in enclosed or partially enclosed spaces. Use them outdoors at least 20 feet from all doors, windows and air vents.
Do not use charcoal grills or propane stoves indoors, even in a fireplace.
Never use the stove or other gas appliances to heat your home.
Do not idle your car, truck or other vehicle in the garage, even if the garage door to the outside is open. Fumes can build up quickly in the garage and living area of your home.
Keep rooms well ventilated.
Read and follow all instructions that accompany fuel-burning devices. Use the proper fuel and make sure there is enough air for ventilation and fuel burning.
Install and maintain a carbon monoxide alarm in your home.
For more information about carbon monoxide poisoning prevention, click here.
As children across North Carolina head back to school this month, the North Carolina Department of Health and Human Services reminds families that vaccinations are an important part of back-to-school success and overall health and well-being.
"Ensuring children are current on their childhood vaccines is essential for both child and family health and well-being," said Dr. Elizabeth Cuervo Tilson, State Health Director and Chief Medical Officer for NCDHHS. "We encourage parents to work with their children’s health care provider or local health department to make sure they’re up to date to protect them from serious disease and help prevent the spread of disease in the classroom and at home."
Vaccine-preventable diseases, such as meningitis, measles, pertussis (whooping cough) and others, are still seen across North Carolina. Keeping children up to date on vaccinations is the best way to keep them healthy and reduce severe illness and unnecessary absences from school. Children who are uninsured can be vaccinated at low or no cost through the Vaccines for Children program, which offers free vaccines to eligible children through 18 years of age.
"Vaccines remain one of the most effective means available to prevent serious illness, hospitalization and death," said Dr. Kelly Kimple, Acting Director of the NCDHHS Division of Public Health. "They help to protect the health of children, their families and the entire community from the spread of these infectious diseases."
Governor Roy Cooper proclaimed August as Immunization Awareness Month in North Carolina. Alongside the proclamation, NCDHHS is partnering with health care providers and stakeholders in a statewide awareness campaign to help ensure school-age children and teens are protected from vaccine-preventable diseases.
"As children, adolescents and young adults are returning to schools and universities, we must remember the critical role of vaccines in preventing illness," said Kenya McNeal-Trice, MD FAAP, President of the North Carolina Pediatric Society. "Well visits, sports physicals, school health assessments and any other health care visit can be used as an opportunity to receive or become up to date on immunizations."
NCDHHS encourages all parents to talk with their child’s health care provider about recommended vaccinations. During that same visit, parents can talk with their physician about the importance of the COVID-19 vaccine and the flu vaccine for their children ages six months and older. Visit this CDC portal for more information about COVID-19 vaccines.
"As children move into their preteen and teen years, they become more susceptible to certain diseases, making it especially important to stay current with immunizations. At the same time, preteens and teens tend to have fewer visits to their doctor’s office, increasing the chance that they are not up to date," said Dr. Garett Franklin President of the NC Academy of Family Physicians. "Make sure our adolescents stay up to date by asking their physician about needed and recommended immunizations."
More information and resources are available for parents and guardians:
In Session Law 2023-134, the North Carolina General Assembly (NCGA) appropriated $5,000,000 in SFY 2024 and $15,000,000 in SFY 2025 in receipts (State funds) from the ARPA Temporary Savings Fund to the Office of Rural Health (ORH) in the Department of Health and Human Services to provide competitive grants to rural healthcare providers for Telehealth related items including:
equipment
high-speed internet access
telehealth-related training to staff and patients
technology equipment to patients
internet service support for patients to help facilitate telehealth access*
other infrastructure needed to establish telehealth services
*Eligible rural healthcare patients can benefit from internet service and associated equipment rentals, including modems, routers, and hotspot devices through the Telehealth Infrastructure grant. To receive this support, patients must meet at least one of the eligibility criteria defined below:
Total household income that is at or below 200% of the federal poverty guidelines or,
Participation in any ONE of these government benefit programs:
Lifeline
Supplemental Nutrition Assistance Program (SNAP)
Medicaid
Federal Public Housing Assistance (FPHA) (including Housing Choice Voucher (HCV) Program (Section 8 Vouchers), Project-Based Rental Assistance (PBRA)/202/811, Public Housing, and Affordable Housing Programs for American Indians)
Veterans Pension and Survivors Benefit
Supplemental Security Income (SSI)
Free and Reduced-Price School Lunch or Breakfast Program including through the USDA Community Eligibility Provision
Federal Pell Grant (current award year)
Special Supplement Nutrition Program for Women, Infants, and Children (WIC)
Priority will be given to independent primary care practices and independent obstetrics and gynecology (OB-GYN) practices.
For more information, eligibility, and other requirements, click here.
Hosted by Dr. Janelle White, Chief Medical Officer of Medicaid and Medicaid colleagues, this month's Back Porch Chat will include important news about NC Medicaid on Tailored Plan Launch, results from the 2022 Annual Health Equity Report, and findings from North Carolina's Healthy Opportunities Pilots Interim Evaluation Report.
Are you registered to vote? If not, instructions are available from the NC State Board of Elections.
Is your voter registration up to date? You can check to make sure their registration information is accurate using the Voter Search tool. Instructions for updating your record are available online as well.
Important General Election dates to note:
Sept. 6, 2024: County boards of elections begin mailing absentee ballots to eligible voters who submitted an absentee ballot request form.
Want to view your sample ballot for the General Election? Registered voters can find their sample ballot in the “Your Sample Ballot” section of their Voter Search profile when they become available.
Don’t forget your photo ID: North Carolina voters will be asked to show photo ID when they check in to vote. Learn more: Voter ID.
GDIT will no longer request supplemental information for undisclosed items discovered during the credentialing and background check process. Failing to inform NC Medicaid through disclosure on the Exclusion Sanction Information page will lead to automatic denial of the application. Depending on the type of application submitted, such as a Re-verification application, additional adverse action can occur up to and including termination of the NCTracks provider record.
When the Exclusion Sanction question asks, “Has the applicant, managing employees, owners, or agents ever...”, it must be answered accurately for anyone listed on the application, and regardless of the length of time since the infraction occurred.
For example, a reportable infraction that occurred five, 10, or even 20 years prior to the application must be disclosed and accounted for with each application submission. In addition, disclosing an infraction once on one application is not sufficient. As long as the applicant, managing employee, owner or agent remains active on the application, disclosure requirements apply for every application wherein the Exclusion Sanction Information page is displayed for response.
For every Exclusion Sanction question answered affirmatively, providers must submit a complete copy of the necessary supporting documentation and a written explanation related to the infraction that is signed and dated within six months of the application date.
This written explanation must be signed by either the individual with the infraction or an Office Administrator (OA) if the infraction is organization related.
All dates must align between the documentation provided and the dates reported in the application.
If this documentation is not included with the application, NCTracks will inform the provider of the exact reason why the application was deemed incomplete to include an itemization of the supporting documentation missing from the application.
Failure to disclose supporting documentation related to an affirmative response will result in a denial of the application.
The U.S. Department of Health and Human Services (HHS), through the Health Resources and Services Administration (HRSA), awarded nearly $9 million to 18 HRSA-funded health centers to improve access to life-saving cancer screenings in underserved communities. Health centers will partner directly with National Cancer Institute-Designated Cancer Centers to expedite patient access to cancer care and treatment. These awards advance the Biden Cancer Moonshot mission to prevent 4 million cancer deaths by 2047 and end cancer as we know it. This effort builds on work supported by the 21st Century Cures Act to expand use of proven cancer prevention and early detection strategies to reduce cancer risk in all populations.
“HHS supports efforts to help people live longer, healthier lives. That’s why we are doing all we can to make cancer prevention and screening services accessible to all Americans,” said HHS Secretary Xavier Becerra. “The funding for health centers announced today is another step towards reducing health disparities across races, ethnicities, genders, and incomes—which is essential to realizing the President’s goal of ending cancer as we know it.”
Two years ago, President Biden and First Lady Jill Biden reignited the Cancer Moonshot and set two national goals: To decrease the cancer death rate by at least 50% over 25 years and to improve the experience of people who are touched by cancer. The Biden-Harris Administration placed a strong emphasis on cancer screening, since Americans missed more than 10 million cancer screenings during the early days of the COVID-19 pandemic and patient outcomes are drastically improved with early detection.
“No matter where you live or what resources you have, everyone should be able to benefit from the tools we have to detect, diagnose and treat cancer before it’s too late,” said HRSA Administrator Carole Johnson. “HRSA is proud to increase our investment in partnerships between our health centers and cancer centers to improve access to live-saving cancer prevention in communities that have been underserved for too long.”
Cancer is the second-leading cause of death in the United States, with approximately 600,000 deaths annually. Appropriate screening and timely follow-up care help to detect cancer early and improve outcomes for patients. However, significant disparities in cancer screening and follow-up care persist, particularly among individuals of different income levels, insurance statuses, and racial or ethnic backgrounds.
HRSA’s Health Center Program is a cornerstone of our country’s health care system, especially for individuals and families who are uninsured, enrolled in Medicaid, living in rural or underserved areas, struggling to afford co-pays, experiencing homelessness, residing in public housing, or having difficulty finding a doctor or paying for care.
CMS issued a final procedural notice outlining a Medicare coverage pathway to achieve more timely and predictable access to certain new medical technologies for people with Medicare.
The new TCET pathway for certain Food & Drug Administration (FDA)-designated Breakthrough Devices increases the number of NCDs that CMS will conduct per year and supports both improved patient care and innovation by providing a clear, transparent, and consistent coverage process while maintaining robust safeguards for the Medicare population.
CMS anticipates accepting up to five TCET candidates per year and, for technologies accepted into and continuing in the TCET pathway, CMS’ goal is to finalize a national coverage determination (NCD) within six months after FDA market authorization.
The Centers for Disease Control and Prevention (CDC) is issuing this Health Alert Network (HAN) Health Advisory to notify clinicians and health departments about the occurrence, geographic spread, and sexually associated human-to-human transmission of Clade I Monkeypox virus (MPXV) in the Democratic Republic of the Congo (DRC). MPXV has two distinct genetic clades (subtypes), and cases of Clade I MPXV have not been reported in the United States at this time (a clade is a broad grouping of viruses that has evolved over decades and is a genetic and clinically distinct group). However, clinicians should be aware of the possibility of Clade I MPXV in travelers who have been in DRC. Clinicians should notify their state health department if they have a patient with mpox-like symptoms, which may include a diffuse rash and lymphadenopathy, and recent travel to DRC. Clinicians should also submit lesion specimens for clade-specific testing for these patients.
Vaccines (e.g., JYNNEOS, ACAM2000) and other medical countermeasures (e.g., tecovirimat, brincidofovir, and vaccinia immune globulin intravenous) are available and expected to be effective for both Clade I and Clade II MPXV infections. However, vaccination coverage in the United States remains low, with only one in four people who are eligible to receive the vaccine having received both doses of JYNNEOS. CDC recommends that clinicians encourage vaccination for patients who are eligible.
To help identify and address health disparities and improve the health of populations that have been historically marginalized, the North Carolina Department of Health and Human Services (NCDHHS) Division of Health Benefits (DHB) developed the 2022 Annual Health Equity Report, which outlines health disparities across the entire NC Medicaid beneficiary population.
The report looks at 50 quality measures and identifies health disparities across eight demographic stratifications (e.g., ethnicity, gender, and disability status). The results are organized into six domains:
member experience,
child and adolescent health,
women’s health,
mental health,
substance use, and
health care utilization.
For 2022, the domain with the largest count of identified disparities was the substance use domain, and the demographic stratifications with the highest count of identified disparities were beneficiaries who identify as having a disability and those with long-term services and support needs.
In addition to identifying health disparities, the 2022 Annual Health Equity Report highlights programs across NC Medicaid that are working towards eliminating health inequities. This report will serve as a tool, alongside other department and division-wide efforts, to identify areas of need and track health disparities over time.
The full report and a six-page brief are available here:
Excessive rains and flooding can cause water in your private well to become contaminated, meaning the water can cause adverse health effects if it is consumed or comes into contact with the skin. NCDHHS recommends the following steps to prepare and protect your private well ahead of adverse weather:
Store adequate bottled water for drinking and cooking. You won't be able to drink, brush teeth or cook with well water until it is tested and found suitable.
Fill up the pressure tank as much as possible.
Turn off the electricity to the well.
If you have an aerobic septic system, turn off the electricity for the system. No special preparations are recommended for conventional septic systems.
If your wellhead does not have a watertight seal, clean off the well casing, cover with a heavy-duty trash bag and secure with waterproof tape.
Locate a nearby water testing lab to obtain sample collection bottles and instructions when it is safe to do so. Often, your local health department can test your water for bacterial contamination. If there is not a health department near you, your county extension agent can help you find a lab.
Locate the log or well report completed when the well was established and store a copy in a safe place that will be accessible if you need to evacuate.
After Hurricane Florence in 2018, nearly 45 percent of wells tested by the State Laboratory of Public Health were found to have bacterial contamination. More than 13% of these wells had detectable E. coli.
After a flood, the following steps can help ensure your well is safe for use:
Do not turn on the electricity to your pump until flood waters recede.
If extensive flooding has occurred, do not drink the water. Use water reserves and bottled water until your well water has been tested and deemed safe for use.
Contact a driller if you think your well will need service immediately after the flood. You can find a list of certified well contractors here.
If you haven't already, find a nearby water testing lab to obtain sample collection bottles and instructions for bacterial contamination. You cannot see, taste or smell bacterial contamination in your well. Often, your local health department can test your water. If there is not a health department near you, your county extension agent can help you find a lab.
If you live near animal feeding operations, agricultural fields where pesticides are applied or industrial chemical factories, you should contact your local health department for additional testing, especially if you smell fuel or chemicals in your water.
If there is bacterial contamination, do not use contaminated water for drinking, cooking, making ice, bathing in any form or washing clothes or dishes. Use an alternative water source until bacteria is no longer detected in your water. Alternative sources include bottled water, a source you know isn't contaminated or boiling your water for five minutes before use.
It is strongly recommended to call your local health department or licensed well driller to shock chlorinate the well if it has been flooded. A water well driller will have access to more effective products and will have equipment and experience that a typical well owner will not have.
For more information about well water and health, click here.
Due to hazardous weather and travel conditions incited by Tropical Storm Debby, Dosher has canceled their August 8th drive-through school supply donation event. This would have been Dosher’s 4th annual “Operation School Supplies,” in which donations are collected for Communities in Schools (CIS) of Brunswick County to support the students that they serve. Dosher encourages community members who had planned to attend the August 8th event to drop off school supply donations at a CIS sponsored “Stuff Our Bus” school supply drive on either August 12th or August 13th at participating Brunswick County Walmart locations, from 10:00am – 4:00 pm each day. The donation site will be a yellow school bus parked outside of the store.
Dosher Memorial Hospital will deliver school supplies collected from their staff members to the yellow school bus at the Southport Walmart on August 13th.
“Dosher Hospital has enjoyed hosting school supply donation events to benefit the students served by CIS for the last three years, and we are grateful for the ongoing support from our community and staff. Despite the weather interfering with our planned event at the hospital, we look forward to helping CIS stuff the bus this Tuesday with the generous donations we have collected from Dosher staff members,” said Dosher President and CEO Lynda Stanley,
Please reach out to the office of Community Relations at Dosher Memorial Hospital at 910-457-3900 with any questions.
As Tropical Storm Debby moves closer to North Carolina, it has the potential to bring heavy rainfall, flash flooding, and isolated tornadoes to the state. In anticipation, the North Carolina Medical Society is offering essential information to ensure you are well-prepared and equipped. These valuable resources are designed to enhance your readiness and improve your response to Debby's potential impacts.
Chief Wellness Officers: Strategizing, Developing, and Implementing
Dr. Christina Bowen, Chief Wellbeing Officer at East Carolina University Health, and President of the Board of Directors for the North Carolina Clinician & Physician Retention and Well-being (NCCPRW) Consortium was recently featured on the Rx for Success Podcast’s, “Life Changing Moments”, hosted by Dr. Dael Waxman.
The podcasts most recent series focuses on Chief Wellness Officers across healthcare systems and discusses how these leaders are strategizing, developing, and implementing innovative solutions to improve the professional lives of physicians at their organizations.
As the second participant in this 4-part series, Dr. Bowen shares her background and the evolution of her role as CWO, and discusses the integration of personal well-being, systemic changes, and a culture of coaching and support.
Click here to listen to Dr. Bowen’s interview, along with the other episodes from the Chief Wellness Officer series.
Hosted by Dr. Janelle White, Chief Medical Officer of Medicaid and Medicaid colleagues, this month's Back Porch Chat will include important news about NC Medicaid on Tailored Plan Launch, results from the 2022 Annual Health Equity Report, and findings from North Carolina's Healthy Opportunities Pilots Interim Evaluation Report.
This spring the North Carolina Clinician and Physician Retention and Well-being (NCCPRW) Consortium announced a new statewide initiative with the Dr. Lorna Breen Heroes’ Foundation, the only non-profit organization exclusively focused on health worker mental health and well-being. ALL IN: Caring for North Carolina’s Caregivers seeks to support the state’s hospitals and health systems in redesigning their workplace environments to help team members feel valued and supported while creating the best environments to deliver safe, quality patient care.
Chip Baggett, JD, CEO North Carolina Medical Society
“This first-of-its-kind consortium has done incredible work to bring physicians, PAs, nurses and health systems together to promote well-being that goes beyond work-life balance for those who are providing care to others,” said Chip Baggett, JD, CEO of the North Carolina Medical Society. “With the launch of this initiative, we are not only acknowledging but taking action to change our system so we can improve the lives of our caregivers and ultimately health outcomes for their patients.”
Hospitals and health systems participating in the initiative commit to:
Make a public commitment to their workforce’s well-being by eliminating local barriers to mental health care access for licensed health workers.
Participate in a digital curriculum to enhance understanding of the drivers of burnout and successful approaches to improve well-being.
Create and implement a 12-month action plan to accelerate systems change to operational and administrative burdens.
This initiative is being launched with a calling to North Carolina hospitals and health systems to remove one of the most substantial causes to health workers’ poor mental health and well-being – the fear of losing their credentials to work due to overly broad and invasive mental health questions on credentialing applications. These questions are stigmatizing and discriminatory, and they often cause health workers to avoid seeking the mental health care they may need. The hospitals and health systems that audit and change language on credentialing applications will be recognized as being ALL IN for prioritizing clinician well-being and be recognized as a Wellbeing First Champion.
Additionally, many state licensure boards include these stigmatizing and invasive questions around mental health in their applications, which determine whether a health worker is licensed to work in a specific state. North Carolina’s attestation model in physician licensing applications, which uses supportive language around mental health, has served as a gold standard for other states to audit and change their applications. By launching ALL IN: Caring for North Carolina’s Caregivers, North Carolina is expanding on its leadership and commitment to support the mental health and well-being of its healthcare workforce.
Corey Feist, JD, MBA, co-founder and CEO, Dr. Lorna Breen Heroes’ Foundation
“By launching this initiative, we are taking an enormous leap forward to ensure North Carolina’s health workers have healthy, supportive work environments and access to the essential mental health resources they deserve,” said Corey Feist, JD, MBA, co-founder and CEO of the Dr. Lorna Breen Heroes’ Foundation. “The state of North Carolina continues to demonstrate leadership in this space and dedication to the well-being of its health workers.”
For hospitals and health systems interested in being recognized as a Wellbeing First Champion, download the Dr. Lorna Breen Heroes’ Foundation’s toolkit to remove intrusive mental health questions from credentialing applications.
About Dr. Lorna Breen Heroes’ Foundation
The Dr. Lorna Breen Heroes’ Foundation’s vision is a world where seeking mental health care is universally viewed as a sign of strength for health workers. We believe every health worker should have access to the mental health care and professional well-being support that they may need, at every moment in their career. We carry out this mission by accelerating solutions, advancing policies, and making connections that put our healthcare workforce’s well-being first. For more information, visit drlornabreen.org.
About North Carolina Clinician and Physician Retention and Well-being (NCCPRW) Consortium
The North Carolina Clinician and Physician Retention and Well-being Consortium (NCCPRW) is a collaborative initiative aimed at identifying and developing strategies to reduce stress and improve well-being among the healthcare workforce at the individual, organizational, and state level. Founded in 2016 in response to concerns raised by the North Carolina Medical Society (NCMS) regarding invasive language in licensing renewal materials, the Consortium has evolved into a proactive force advocating for the mental health and wellness of healthcare professionals. In 2024, the Consortium transitioned into a 501(c)(3) nonprofit organization to further its mission.
UNC Hospitals in Chapel Hill, UNC Health Rex in Raleigh and UNC Health Pardee in Hendersonville have received top 5-Star ratings from the Centers for Medicare and Medicaid Services (CMS), which measures hospital quality and safety to help consumers make informed choices.
The latest CMS hospital ratings, which were posted on the CMS website in late July, use a wide range of publicly available data in categories that include mortality, safety of care, readmissions, timely and effective care, and patient experience. CMS provides the star ratings to help patients make decisions about where to get health care and encourage hospitals to improve the quality of care they provide.
Among UNC Health hospitals:
UNC Hospitals maintained its 5-Star rating
UNC Health Rex maintained its 5-Star rating
UNC Health Pardee improved from 4 Stars to 5
“UNC Health strives to lead the way in providing the very best care to the people of North Carolina,” said Dr. Wesley Burks, CEO of UNC Health. “It’s the heart of our mission and the daily focus of our dedicated teammates. We’re especially proud to see several of our locations recognized with such high star rankings from CMS.”
To learn more about CMS hospitals ratings or to compare the ratings of other hospitals, visit the Hospital Compare website.
To help set the stage for the anticipated year-end push to get federal health policy issues across the finish line in Congress, a contingent from North Carolina traveled to Capitol Hill last week to help build urgency around key, pending bills. Their Hill visits were part of the Alliance of Specialty Medicine’s advocacy conference, which drew participation from across the country.
The group included . . .
Eileen Raynor, MD – Pediatric Otolaryngologist / Duke President / NC Medical Society
Lynn Damitz, MD – Plastic Surgeon / UNC-Chapel Hill
Geoffrey Rose, MD – Cardiologist / Atrium
W. Alan Skipper, CAE – NC Medical Society
The group visited all of our Senate and House offices to address legislation of great consequence to North Carolina physicians and practices. The most urgent message delivered was that Congress needs to act now to avert another cut in Medicare physician payment. A 2.8% payment cut is on the 2025 horizon, which would come on the heels of successive annual cuts for the past four years. When adjusted for inflation, physicians have seen a 29% cut in Medicare payment since 2021, while practice expenses have continued to rise.
Legislation specifically addressed in meetings with congressional offices include:
Medicare Physician Payment Reform
H.R. 6545 – the Physician Fee Schedule Update and Improvements Act
H.R. 2474, the Strengthening Medicare for Patients and Providers Act
H.R. 6371, the Provider Reimbursement Stability Act
S. 1302 - the Resident Physician Shortage Reduction Act
H.R. 2389 - the Resident Physician Shortage Reduction Act
The NCMS continues to engage with state and national partners to advance our congressional advocacy agenda, especially Medicare payment reform. Presently, our topline issue is the pending 2.8% Medicare payment cut that looms for the coming year. You can helpthat effort! Please reach out to your members of the Senate and House using the American Medical Association’s portal.
Your engagement matters.
Do you know your state and federal legislators? More importantly, do your legislators know you? The NCMS can help you connect with policy makers as a constituent and advocate!
STAY OUT OF FLOODWATER, AND DON'T DRIVE THROUGH FLOODED AREAS.
As of this posting, the National Hurricane Center places Debby's newest path as going straight through North Carolina. Governer Roy Cooper declared a State of Emergency ahead of the expected impact. The system will bring significant rain to the state with the potential of massive flooding in many areas. Floodwater can not only be dangerous but can also put you at risk of injuries or diseases.
Don't drive in flooded areas.
Always follow warnings about flooded roads.
Don't drive in flooded areas—cars or other vehicles won't protect you from floodwaters. They can be swept away or may stall in moving water.
(image credit: CDC)
For more information on staying safe from floodwater, click here.
Sunscreen has been a hot topic on social media recently with celebrities, bloggers, and content creators warning of the perils of frequent sunscreen use. While fear-tactics may cause you to worry, scientific research shows the benefits of protecting your skin with sunscreen.
Humans have been protecting their bodies from the sun since the beginning of time. Ancient Egyptians used rice bran, jasmine, and lupine to block out the sun’s rays. Ancient Greeks slathered on olive oil for exposure and after-care. Scientists have revolutionized how we care for our skin in the sun with the introduction of modern creams, sprays, and lotions, but many consumers believe the risk outweighs the benefit.
While our ancestors spent a significant amount of time outside, the typical life expectancy then was less than half of today’s according to Our World in Data. The average age for a skin cancer diagnosis is 66, more than double the average age of 30 in 1770. The sun’s true damage to their bodies would have gone undetected with them passing away before cancer had a chance to take its toll. The indoor tanning boom of the 1970s is a contributor to an increase in skin cancer, along with the thinning of the ozone layer, allowing more UV rays to pass through. Choosing not to use sunscreen puts you at risk for cancer, sunburn, and other sun-related illnesses.
According to the Food & Drug Administration (FDA), genetic and health factors also play a role in the harmfulness of UV rays. Take extra precaution if you have:
Pale skin
Blonde, red, or light brown hair
Been treated for skin cancer
A family member who has had skin cancer
Take certain medications (consult with your doctor)
How Does Sunscreen Protect the Skin? “Sunscreen forms a protective barrier on your skin, reducing the amount of UV radiation that reaches the deeper layer of your skin. This helps prevent sunburn and skin damage and reduces the risk of skin cancer,” explained Landon Marshall, FNP-C, of Iredell Health System’s Family Care Center of Taylorsville. “There are two main types of UV rays that reach our skin:
UVB rays are responsible for causing sunburn. Sunscreen with a high sun protection factor (SPF) helps to block or absorb these rays before they can penetrate the skin and cause damage.
UVA rays also damage the skin, leading to premature aging and an increased risk of skin cancer. Broad spectrum sunscreen protects us against both UVA and UVB rays.”
There are two types of sunscreen protection: chemical and mineral. Chemical sunscreens absorb UV rays and neutralize them. Mineral sunscreens create a protective barrier on the skin and bounce UV rays away. Zinc oxide and or titanium oxide are typical ingredients found in mineral sunscreens.
Should I Worry About Sunscreen Causing Cancer? “Some people may have concerns about the chemicals in sunscreen and their potential impact on health, including the risk of cancer. If this is one of your concerns, I would encourage you to weigh the potential risks against the known benefits of using sunscreen and the harmful effects of UV radiation,” said Marshall.
From the American Academy of Dermatology (AAD):
“A recent study by the FDA looked at four sunscreen ingredients and concluded that absorption of these ingredients into the body supported the need for additional research to determine if the absorption has any effects on a person’s health. As the researchers pointed out, just because an ingredient is absorbed into the bloodstream does not mean that it is harmful or unsafe.
Skin cancer is the most common cancer in the U.S., and unprotected exposure to the sun’s harmful ultraviolet rays is a major risk factor for skin cancer. The AAD remains committed to supporting and enhancing patient care. If you are concerned about the safety of the ingredients in your sunscreen, speak with a board-certified dermatologist to develop a sun-protection plan that works for you. For more information, check out aad.org/media/stats-sunscreen.”
What is SPF Anyways? A common misconception is the higher the SPF, the longer a person can go without reapplying. This is false.
According to the FDA, “SPF is a measure of how much solar energy (UV radiation) is required to produce sunburn on protected skin (i.e., in the presence of sunscreen) relative to the amount of solar energy required to produce sunburn on unprotected skin. As the SPF value increases, sunburn protection increases.”
SPF protects against UVB rays, which is why it’s important to choose a product labeled “broad spectrum” that protects the skin from both UVA and UVB rays. SPF 15 filters 93% of the sun’s UVB rays while SPF 30 filters 97%. When choosing a sunscreen, the AAD recommends choosing one with an SPF of 30 or higher and reapplying every two hours. It’s important to note that no sunscreen will filter 100% of the sun’s UVB rays, so pairing sunscreen with hats, sunglasses, and protective clothing is the best way to practice sun safety. It’s important to reapply:
Every two hours
After toweling off
When sweating
After being in water
Is Sunscreen Healthy or Hazardous? Bottomline: Protecting your skin with sunscreen is a safe and effective way to prevent burns, cancers, and other sun-related illnesses. It’s important to do personal research and speak with your healthcare provider about a sun-safety plan that’s right for you.
“I would say that sunscreens are regulated by health organizations to ensure they are safe for use and overall, the risk of developing any kind of adverse effect from the use of sunscreen is much lower than the risk of developing skin cancer from unprotected UV exposure,” said Marshall.
It’s important to keep your skin safe from harmful UV rays. Slather on the sunscreen and suit up- your skin will thank you later. [source]
Alamance Regional Medical Center in Burlington, Annie Penn Hospital in Reidsville and The Moses H. Cone Memorial Hospital in Greensboro have received a combined7 American Heart Association Get With The Guidelines® achievement awards. The honors are for demonstrating commitment to following up-to-date, research-based guidelines for the treatment of stroke. Doing so ultimately leads to more lives saved, shorter recoveries and fewer return trips to the hospital.
Get With The Guidelines puts the expertise of the American Heart Association and American Stroke Association to work for hospitals nationwide. This helps ensure patient care is aligned with the latest research and guidelines. Get With The Guidelines - Stroke is an in-hospital program for improving stroke care by promoting consistent adherence to these guidelines, which can minimize the long-term effects of a stroke and even prevent death.
“Cone Health is committed to improving patient care by adhering to the latest treatment guidelines,” says Robert Hickling, executive director, Cone Health Stroke Center. “Get With The Guidelines makes it easier for our teams to this proven information to work on a daily basis, which studies show can help patients recover better. The end goal is to ensure more people in Greensboro, Reidsville, and Burlington experience longer, healthier lives.”
Effective August 1, 2024, NC Medicaid is removing copayment requirements for opioid antagonists, nicotine replacement therapy and medications used to treat opioid use disorder. This change applies to both NC Medicaid Direct and NC Medicaid Managed Care beneficiaries who are covered under the Outpatient Pharmacy benefit.
Currently, an eligible Medicaid beneficiary who receives prescribed drugs is required to pay a $4 copay for each prescription received unless they are exempt for one of the reasons listed in the Outpatient Pharmacy Clinical Coverage Policy No. 9, which is available on the Program Specific Clinical Coverage Policies page.
The exemption, effective August 1, 2024, helps to ensure beneficiaries living with nicotine dependence or opioid use disorder (including emergency treatment of known or suspected opioid overdose) do not face financial barriers when obtaining these medications from outpatient pharmacies. Additionally, this exemption supports public health efforts to increase access to substance use disorder treatment.
The North Carolina Department of Health and Human Services will host a live Spanish-language Cafecito and tele-town hall on Tuesday, August 6, from 6 to 7 p.m., to discuss who is newly eligible for Medicaid under expansion, ways to apply, how to access application support in Spanish and which qualified immigration statuses are eligible for health care coverage.
Jennifer Platts, Communications Specialist, NC Medicaid
Sarai Serrano, NC Medicaid Expansion Program Manager, Hispanic Federation
More people ages 19 through 64 years can now get Medicaid in North Carolina as of Dec. 1, 2023, including thousands of individuals who are part of the Hispanic and Latino community. Many people who now qualify for Medicaid under expansion work in child care centers, grocery stores, nursing homes, clothing stores, restaurants and other industries who may not have comprehensive health insurance through their jobs. People who did not qualify for Medicaid in the past may now be eligible, regardless of whether they have children or a disability. Some non-U.S. citizens with qualified immigration status in North Carolina can also get health care coverage through Medicaid.
Cafecito and tele-town hall panelists will discuss the following:
Where to find Medicaid resources and application support in Spanish
Impacts of Medicaid expansion on health coverage for the Hispanic and Latino community in North Carolina
While more than half a million newly eligible North Carolinians have already enrolled in Medicaid, nearly 100,000 who may be eligible have not yet applied. State and local support teams are available to provide confidential support and help Spanish-speaking communities better understand their health care coverage options, complete Medicaid applications and navigate enrollment.
The Cafecito will stream live from the NCDHHS Facebook, X (Twitter) and YouTube accounts, where viewers can submit questions. The event also includes a tele-town hall, which invites people by phone to listen in and submit questions. People can also dial into the event by calling 855-756-7520 Ext. 108572#.
NCDHHS’ Cafecito’s and tele-town halls are part of the state’s ongoing public efforts to ensure equitable access to timely health information, including Medicaid enrollment updates and resources to help North Carolinians find health care coverage.
El Departamento de Salud y Servicios Humanos de Carolina del Norte (NCDHHS) organizará un Cafecito, una conversacion en vivo y en español el martes 6 de agosto, de 6 a 7 p.m., para hablar sobre la nueva elegibilidad por medio de la expansión de Medicaid, las formas de aplicar, cómo acceder a apoyo para la aplicación en español y cuáles estatus migratorios calificados son elegibles para la cobertura de atención médica.
Los panelistas del evento incluyen:
Carolina Siliceo Perez, MLAS, Gerente de proyectos de política y estrategia Latinx/Hispana para NCDHHS
Jennifer Platts, Especialista en comunicación, Medicaid de Carolina del Norte
Sarai Serrano, Gerente del programa de expansión de Medicaid de Carolina del Norte, Hispanic Federation.
A partir del 1 de diciembre de 2023, más personas entre 19 y 64 años han podido obtener Medicaid en Carolina del Norte, incluidas miles de personas que forman parte de la comunidad hispana y latina. Muchas personas que ahora califican para Medicaid bajo la expansión trabajan en centros de cuidado infantil, supermercados, hogares de ancianos, tiendas de ropa, restaurantes y otras industrias que pueden no tener un seguro de salud integral a través de su empleador. Las personas que antes no calificaban para Medicaid ahora pueden ser elegibles, independientemente de si tienen hijos o una discapacidad. Algunos ciudadanos no estadounidenses con estatus migratorio calificado en Carolina del Norte también pueden obtener cobertura de atención médica a través de Medicaid.
Los panelistas del Cafecito y el evento en vivo hablaran sobre los siguientes:
Qué servicios de salud están cubiertos por Medicaid
Dónde encontrar recursos y apoyo para la aplicación de Medicaid en español
Los impactos de la expansión de Medicaid en la cobertura de salud para la comunidad hispana y latina en Carolina del Norte
Más de medio millón de nuevas personas elegibles en Carolina del Norte ya se han inscrito en NC Medicaid, pero casi 100,000 que pueden ser elegibles aún no han aplicado. Equipos de apoyo estatal y local están disponibles para proporcionar apoyo confidencial y ayudar a las comunidades de habla hispana a comprender mejor sus opciones de cobertura de salud, completar las aplicaciones de Medicaid y navegar el proceso de inscripción.
El Cafecito se transmitirá en vivo desde las cuentas de Facebook, X (Twitter) y YouTube de NCDHHS, donde los espectadores podrán enviar preguntas. El evento también incluye una telecomunicación en vivo que invita a las personas a escuchar y enviar preguntas por teléfono. También se puede participar en el evento llamando al 855-756-7520 Ext. 108572#.
Los Cafecitos de NCDHHS son parte de los esfuerzos públicos continuos del estado para garantizar un acceso equitativo a información de salud oportuna, incluyendo actualizaciones de inscripción en Medicaid y recursos para ayudar a los habitantes de Carolina del Norte a encontrar cobertura de atención médica.
Stop the Revolving Door: Recruiting and Retaining High-Performing Employees
August 13, 2024 | noon-1 p.m.
In this webinar led by Katie Lawrence, MHA CMPE, leaders will learn five keys to curating a culture that retains top talent and become a workplace that people seek out. An environment that draws new people in and invites them to stay is never just an accident. Leaders must intentionally decide to learn and leverage best practices.
Objectives include:
Implement best practices for selecting interview questions and onboarding new employees.
Recognize when and how to use emotional intelligence to enhance one aspect of workplace culture.
Leverage process improvement and technology to improve workplace culture.
The U.S. Department of Health and Human Services, through the Centers for Medicare & Medicaid Services (CMS), issued a final rule updating Medicare payments and policies for inpatient hospitals and long-term care hospitals. The rule improves the health of people with Medicare by addressing key social determinants of health and strengthening emergency preparedness. The fiscal year (FY) 2025 Inpatient Prospective Payment System (IPPS) and Long-Term Care Hospital Prospective Payment System (LTCH PPS) rule builds on the Biden-Harris Administration’s work to support the health of historically underserved and under-resourced communities and promote value-based care.
Get additional information, including rate Increases, resources for Underserved Patients and Communities, and more, here.
Governor Roy Cooper joined North Carolina Department of Health and Human Services leadership and a representative from Walgreens for an announcement on Medicaid coverage in Chapel Hill. As part of NCDHHS and the Governor’s continued work to expand access to reproductive health services, NC Medicaid will begin covering over-the-counter contraception in pharmacies across the state. Starting Thursday, August 1, 2024, the oral contraceptive Opill will be available through local and retail pharmacies without a prescription, at no cost for NC Medicaid beneficiaries. Opill is the first over-the-counter oral contraception that has been approved by the U.S. Food and Drug Administration.
"North Carolina is working to expand access to health care and that includes the freedom to make decisions about family planning," said Governor Cooper. "Making birth control easier to get is an important goal and I’m glad that NC Medicaid can take this step."
"Our goal is to ensure everyone has access to the right contraception and reproductive services at the right time in their community," said NC Health and Human Services Secretary Kody H. Kinsley. "This new coverage is part of our ongoing work to invest in child and family well-being by increasing access to health care and ultimately improving maternal and infant outcomes."
Expansion of contraceptive services allows Medicaid beneficiaries better access to health care by reducing barriers to contraception medication, such as cost and the need for a prescription from their health care provider. Medicaid beneficiaries will be able to get Opill over the counter from Medicaid-enrolled pharmacies who will be able to submit the claim for reimbursement.
"We are so grateful to the pharmacies and pharmacists who are partnering with us in this critical work to expand access to contraception and reproductive health services," said State Health Director and Chief Medical Officer Dr. Elizabeth Cuervo Tilson. "This new coverage by NC Medicaid demonstrates our commitment to continue to remove barriers to contraception and ensure North Carolinians have access to the services they need to make the best decisions about their health and life."
Opill over-the-counter coverage builds on NCDHHS’ ongoing work to ensure more North Carolinians have access to reproductive health services. Prior efforts include the implementation of pharmacist-initiated contraception, through which pharmacists can provide counsel about many options for prescription contraception, initiate a prescription and dispense contraception, and connect people to ongoing care if needed. Community access to contraception is particularly important in rural areas that have fewer providers and are considered maternal health and contraceptive deserts.
North Carolina Session Law 2021-110/HB 96 grants authority to pharmacists to prescribe a variety of contraception under protocols approved by the NC Board of Pharmacy and the NC Medical Board. NC Medicaid began enrolling pharmacists as providers in January 2024. To date, there are more than 330 retail and commercial pharmacies in 92 counties providing contraceptive services. The Department will continue to work to expand the level of access to contraceptive services in communities statewide.
More information about coverage for Opill is available in the NC Medicaid bulletin. To find a pharmacy providing pharmacy-initiated contraceptive services in North Carolina, visit ncpharmacyfinder.com.
The North Carolina Medical Board is seeking applicants to fill a vacancy for a licensed perfusionist on the Board’s Perfusionist Advisory Committee.
The appointment is for a three-year term ending October 31, 2027. The appointed perfusionist will be eligible to serve an additional three-year term after the completion of the first term.
Applicants must have an active, non-limited license to practice perfusion and no public disciplinary actions with the Board or any other professional licensing board within the past 10 years. Committee members receive a per diem and reimbursement for travel and subsistence as provided in G.S. 93B 5.
Interested applicants should submit a cover letter expressing interest in serving on the Committee, a current curriculum vitae or resume, and two letters of recommendation from individuals familiar with the applicant’s practice of perfusion.
Submit application materials by September 1, 2024, to: [email protected].
Please share your stories here on how corporate interventions in medicine have impacted you and your practice. This includes private equity acquisitions, noncompete agreements, management service organizations, and any business intervention that has impacted your ability to practice medicine.
Millions of low- and middle-income North Carolinians are one step closer to medical debt relief. The U.S. Centers for Medicare and Medicaid Services (CMS) approved on Friday, July 26 Governor Roy Cooper and the NC Department of Health and Human Services' plan to use the state's Medicaid program to incentivize hospitals to relieve more than a decade of existing medical debt for eligible North Carolinians and prevent accumulation of new debt going forward.
NCDHHS will now begin working with hospitals to implement the program, which has the potential to relieve a potential $4 billion in existing medical debt for people and families across the state.
"Unlike most other debts, medical debt is not intentional because people don't choose to get seriously ill or have an accident," said North Carolina Governor Roy Cooper. "Medical debts are often beyond people's ability to pay, ruining their credit, keeping them from getting credit cards, loans and jobs and sometimes driving them into bankruptcy. That's why we're working with hospitals and federal partners to help relieve the burden of medical debt for North Carolina families."
"Many people struggle with the burden of medical debt, which can cause them to hold off on getting the essential health care and services they need," said NC Health and Human Services Secretary Kody H. Kinsley. "This debt relief program is another step toward improving the health and well-being of North Carolinians while supporting financial sustainability of our hospitals."
Each hospital in North Carolina can elect whether to participate in the program. Hospitals that choose to meet the eligibility conditions, including medical debt relief, will receive a higher level of Medicaid reimbursement under the Healthcare Access and Stabilization Program (HASP). Hospitals that choose not to implement the policies are eligible for base HASP payments.
Hospitals that opt in must implement the following policies as a condition of eligibility for enhanced HASP payments:
Relieve all medical debt deemed uncollectible dating back to Jan. 1, 2014, for any individuals not enrolled in Medicaid with incomes at or below at least 350% of the federal poverty level (FPL) or for whom total debt exceeds 5% of annual income.
Relieve all unpaid medical debt dating back to Jan. 1, 2014, for individuals who are enrolled in Medicaid.
Provide discounts on medical bills of between 50-100% for patients with incomes at or below 300% FPL, with the amount of the discount varying based on the patient's income.
Automatically enroll people into financial assistance, known as charity care, by implementing a policy for presumptively determining individuals eligible for financial assistance through a streamlined screening and income validation approach.
Not sell any medical debt for consumers with incomes at or below 300% FPL to debt collectors.
Not report a patient's debt covered by these policies to a credit reporting agency.
Participating hospitals will highlight all outstanding debt owed by current Medicaid enrollees, dating back to Jan. 1, 2014. Other individuals who are not enrolled in Medicaid but have incomes less than or equal to 350% of the FPL, currently $90,370 for a family of three, may also qualify for medical debt relief. Patients of participating hospitals will not need to take any actions to benefit from medical debt relief. The goal of the program is for eligible North Carolinians to begin to see relief for existing medical debt over the next two years.
NCDHHS has partnered with Undue Medical Debt to support participating hospitals and help them identify medical debt that is eligible for relief. Additional information is available in the Frequently Asked Questions on North Carolina medical debt relief.
Grab your party hats and noisemakers and let’s celebrate!
Maureen L. Aarons, MD
Brian C. Adair, MD
Danielle D. Adkins, PA-C
Asma Afzal, MD
Onyinyechi B. Agbara, MD
Daniel J. Albright, MD
James F. Alderman, MD
Kyle A. Aldinger, MD
Andrew H. Allen, PA-C
Elms L. Allen, MD
Christian G. Anderson, MD
Sayeh S. Araghi, PA-C
Jihad O. Arteh, MD
Gale J. Ashley, MD
Kim L. Askew, MD, FAAP
Inad B. Atassi, MD
William S. Atkins, MD
Clinton K. Atkinson, MD, FACS
Samuel M. Atkinson, Jr., MD
Victor K. Au, MD
Hitesh Avaiya, MD
Leanne Avery, PA-C
Hima Bindu R. Avutu, MD
Mofoluwake O. Awe, MD
Ndidi N. Azikiwe, MD
Adam G. Back, MD
Jack L. Bagley, PA
Jodi L. Bailey, MD
David W. Baker, III, MD
Rachel T. Baldwin, MD, MPH
Robert F. Barbe, MD
John V. Barrord, MD
Paul K. Bates, Jr., MD, FAAP
Mary John Baxley, MD
Adrienne C. Bean, MD
Wayne Beauford, MD
Octavian M. Belcea, MD
Sharon A. Belflowers, PA-C
Broderick C. Bello, MD
Lisa Bellofiore-Plonski, MD
Carlos F. Bendfeldt, MD
John D. Benson, MD
Alexandra D. Bentley, MD
Ralph L. Bentley, MD
Susan M. Berendzen, MD
Danilo R. Bernardo, MD, FACP
Shilpa Bhardwaj, MD
Vishal B. Bhuva, MD
Michael J. Bianconi, MD
Holly Biola, MD, MPH, FAAFP
Jenna E. Black, MD
Aaron M. Blackshaw, MD
Gerald W. Blake, MD
Jeffrey C. Blum, MD
O. Robert Boehm, MD, PhD
John P. Booker, Jr., MD
Edward H. Bossen, MD
Lynneice L. S. Bowen, MD
Randall B. Bowen, MD
Karl F. Bowman, Jr., MD
James F. Boyd, MD
Sabrina A. Boyte, PA-C
Melissa M. Braunsteiner, MD
Wilburn O. Brazil, Jr., MD
William M. Brinkley, Jr., MD
Amy S. Brooks, DDS, MD
Werner C. Brooks, MD
Sandra M. Brown, MD
Joel E. Bruce, MD
Kofi Bruce-Mensah, MD, MBA, MS
Scott H. Brundle, MD
J. Scott Bryson, MD
John E. Buenting, MD
Bryan C. Bunn, MD
Paul A. Buongiorno, MD
Woodward Burgert, III, MD
Shawn T. Burgess, MD
Eric S. Burgon, MD, DDS
Thomas E. Burkart, MD
Kristen A. Burke, PA-C
E. Edward Burton, Jr., MD
Marcella M. Butler, MD
Debra L. Bynum, MD
David E. Byrd, MD
Thomas H. Byrnes, Jr., MD
Claudia T. Cadet, MD
Brian H. Camp, DDS, MD
Manuel O. Campano, MD
William E. Campbell, Jr., MD
Kenneth P. Carlson, MD
Stephanie D. Carperos, MD
Henry J. Carr, Jr., MD
Michael J. Carroll, PA-C
Jean W. Carter, MD
Timothy R. Carter, MD
Cornelius F. Cathcart, MD
R. Lamont Cathey, MD
Pamela B. Cavanaugh, MD
Dan Chaksupa, MD
Robert E. Chambers, MD
Daniel R. Champey, MD
C. Peter Chang, MD
Shailendra S. Chauhan, MD
Swapna Chenna, MD
Karl S. Chiang, MD
Karen N. Chilton, MD
Hira Choudhry, MD
Wan S. Chung, MD
W. Tucker Cline, MD
J. Thaddeus Coin, MD, PhD
Emily H. Cole, PA-C
T. Boyce Cole, MD
Robert E. Coles, MD
H. Christopher Coley, MD
Ryan D. Collins, PA-C
Scott V. Connelly, MD
Erin L. Cook, MD
Paul P. Cook, MD
Domagoj Coric, MD
Jamey L. Cost, MD
Stuart W. Couch, MD
R. Lee Cox, MD, FACS
Stanley C. Cox, III, MD
Matthew D. Crawford, MD
Robert C. Crawford, Jr., MD
Susan L. Crittenden, MD
William M. Crutchfield, MD
Jeremy F. Cuda, MD
Walton W. Curl, MD
D. Patrick Currie, MD
Brian M. Curtin, MD
Boris Cvetkovski, MD
Vincent P. Dahringer, MD
Cheryl J. Davis, MD
Grace M. Davis, PA-C
Heather L. Davis, DO
Teneisha C. G. Davis, MD
W. Bradley Davis, MD
Howard G. Dawkins, Jr., MD
Jacquia F. De La Cruz, MD
A. Richard De Sandre, MD, FACS
Alberto J. d'Empaire, MD
Gurvinder S. Deol, MD
Joseph S. DeRaddo, MD
Theodore S. Derse, MD
Maria L. DeSantis-Wilcox, PA
Jonathon G. Dewald, MD
David L. Dill, MD
Daniel C. Dillon, MD
Brian D. Donoghue, MD, FACEP
Margaret R. Donohoe, MD
Margaret J. Dorfman, MD
H. Duncan Dorris, Jr., MD
Memory E. Dossenbach, PA-C
Thomas H. Douglas, MD
Dalton E. Dove, MD
Hugh T. Dowlen, MD
Gregory J. Dray, MD
Laura E. Dressel, MD
Olly C. Duckett, MD
Harold C. Dufour, MD
Priti Duggal, MD
Gina L. N. Duncan, MD
S. Bryan Durham, MD
Marcus A. Earle, DO
James S. Easterbrook, MD
Donna H. Edwards, MD
Chad R. Eller, MD
J. Kent Ellington, MD
Henry J. Elsner, MD, FACS
Robert D. Ensor, MD
Thomas C. Eshelman, MD
Scott M. Eskildsen, MD
Mohammad A. Esmadi, MD
Meagan E. Evangelista, MD
Scott N. Fairbrother, MD
Jenna L. Falcinelli, MD
William L. Falls, MD
John K. Farrington, MD
Clinton E. Faulk, MD
Max H. Faykus, Jr., MD
Alan G. Finkel, MD, FAAN, FAHS
Richard C. Finn, MD
D. Russell Fisher, MD
Christina M. Flannelly, MD, FAAP
Lisa C. Fleck, PA-C
Marisa C. Flores, MD
Herbert M. Floyd, MD
Lisa M. Foglia, MD
Rita I. Fontaine, PA-C
Daniel J. Forest, MD
Jamie L. Fountain, MD
Reginald J. Fowler, MD
David D. Fraser, MD
Ray M. Freeman, MD
Sascha Frey, MD
Julie M. Fry, PA-C
Kim M. Fujinaga, MD
Molly L. Fuller, MD
Imre Gaal, Jr., MD
Suchita B. Gade, MD
Mark W. Galland, MD
Charles B. Gantt, Jr., MD
Rama G. Garimella, MD, FACC
Susan T. Garrett, MD
Richard S. Gelber, MD
Paul Geniec, MD
Laura I. Gerald, MD, MPH
Ronald W. Gerbe, MD
Jennie M. Gillespie, DO
Dennis E. Giordano, MD
John G. Giragos, MD
Ronald P. Glinski, MD, PhD
Thomas M. Golden, MD
Bonnie J. Goodwin, MD
Michael A. Gordon, MD
Daniel Gottovi, MD, FCCP
Lauren P. Gotwald, MD
James M. Granfortuna, MD
Craigan L. Gray, MD, MBA, JD
Katherine V. Grette, MD
William R. Griffin, Jr., MD
Nicholas B. Grissom, MD
Jeffrey L. Gross, MD
Ned J. Gross, MD
C. T. Gualtieri, MD
Robert C. Gunther, MD
Robyn Guo
Michael D. Gwinn, MD
Catherine A. Haggart, PA-C
Cornelia S. H. Hahn, MD, PhD
Gregory G. Hall, MD
Tara L. Halpin, PA
J. Nathaniel Hamilton, MD, FACS
Robert E. Hammonds, MD
George L. Hamrick, Jr., MD
Jason P. Handler, MD
Scott Q. Hannum, MD
Curtis A. Hanson, MD
David M. Hardaway, MD
Christina Hardin-Dial, MD, FAAP
Thomas S. Harle, MD
Jeremy L. Harless, PA-C
Keith W. Harper, MD
Lonnie C. Harrell, III, MD
Sunit P. Harris, MD
John L. Harshbarger, MD
Alexander C. Hattaway, III, MD
Bennett A. Hayes, Jr., MD
Jessica C. Heestand, MD
Janice M. Helm, PA-C
Jasmine P. Hemmings, PA-C
Robert C. Hendel, MD
Joshua M. Henderson, PA-C
John O. Herlong, MD
Alexis B. Hess, MD
Docia E. Hickey, MD
Edward F. Hill, MD
Gregory C. Hinn, MD
Jenny L. Hinson, MD
Todd N. Hodges, MD
Lewis R. Hodgins, MD
Theodore F. Hoffman, Jr., MD
Michael K. Hoger, DO
Robert J. Holmes, MD
Douglas E. Holt, MD
Boyd K. Honeycutt, MD, MBA, FACP
Travis C. F. Honeycutt, MD
Timothy S. Howard, MD
H. Slade Howell, Jr., MD
Olson Huff, MD
Allen W. Huffman, Jr., MD
Charles S. Hultman, MD
Thomas H. Hunt, MD
Justin B. Hurie, MD
Obinna O. Ikwechegh, MD
Jirair A. Injejikian, MD
Edward K. Isbey, Jr., MD
Daniela T. Ivanova, MD
David S. Jackson, Jr., MD
Anshu K. Jain, MD
Bennie L. Jarvis, MD
Michele T. Jedlica, MD
Jennifer L. Jenkins, PA-C
Travis C. Jenkins, MD
Myung K. Jeon, MD
Kathryn B. Jeutter, PA-C
Allen M. Johnson, MD
Dennis R. Johnson, MD
Nell B. P. Johnson, MD
Theresa S. Johnson, MD, FACOG
Carol A. Johnston, MD
William W. Johnston, MD
Frederick Scott Jones, MD
H. Michael Jones, MD
John S. Jones, DO
L. R. Jones, MD
Diya T. Jost, MD
Kyle M. Judkins, DO
Theresa A. Kallman, MD
David E. Kang, MD
Seth A. Kaplan, MD
Lisa Kaufmann, MD
Robert M. Kennedy, IV, MD
Ioanna G. Kessler, DO, FACOFP
Jeffrey P. Keverline, MD
Bilal Khalid, MD
Dalia A. Khalifa, MD
Tahuriah G. Khan, DO
Mayuri L. Khatri, MD, FAAP
Daniel A. King, PA-C
Susan S. Kirsch, MD
Mark H. Knelson, MD
Christopher B. Komanski, MD
Ramesh B. Konduru, MD
John B. Konefal, MD
Doria H. Kosmala, PA-C
Stephen I. Kramer, MD
Jan Kriska, MD
Frederick G. Kroncke, Jr., MD
Theresa B. Kubicki, PA-C
Kenneth R. Kubitschek, MD
David C. Kwee, MD
Michael D. Kwong, MD
Suman Lamsal, MD
Darryl L. Landis, MD
Jason E. Lang, MD
Michael C. Lang, MD
Thomas E. Lawrence, MD
Rusty J. Lee, MD
Donald L. Lendle, MD
Jeffrey P. Lin, MD
Shau-Shau Lin, MD
Allison A. Linton, PA
Perry E. Little, MD
Brooke E. Livingston, DO
Victoria R. Locklear, PA-C
Thomas D. Long, Jr., MD
Fernando A. Lopez, MD
Melissa V. Lowe, MD
Tiffany N. Lowe-Payne, DO
Laura J. Luckadoo, MD
Eric J. Luk, MD
Gaurav Luther, MD
Michael W. Madsen, MD
Scott R. Mahanty, MD
Marc A. Mancuso, MD
Rebecca L. Manganello, DO
Allen F. Marshall, MD
Holly R. Martin, PA-C
Paola A. Matheus, MD
Kacie S. Matthews, PA
Gerri L. Mattson, MD, MSPH, FAAP
David R. Maynard, MD
Carmen C. P. Mayo, PA-C
Jonas J. McAlarney, MD
Beck D. McAllister, MD
James C. McCabe, MD
Chad S. McCain, DO
Kevin C. McCammack, MD
Samantha L. O. McClease, MD, FAAP
William B. McCrea, MD
Erin C. McCrum, MD
Peter McIlwaine, PA-C
Angus G. McInnis, MD
Frederick L. McIntyre, Jr., PA-C
William D. McKeown, MD
Stephen M. McNeill, MD
Sheri R. Meinert, PA-C
Murali Krishna Meka, MD
Karla L. Mendoza Rodriguez, PA-C
Michael J. Menz, MD
Nicole M. Merli, MD
Virgil M. Messer, MD
Sarah M. Messersmith, MD
Doreen R. Messick, MD
Daniel K. Messner, MD
April M. Miller, MD
Mark F. Miller, MD
Robert A. Millet, MD
Andrew V. Moczula, MD
Rasheeda T. Monroe, MD
Lawrence A. Montalto, DO
Gustavo S. Montana, MD
Katharine S. Moorehead, MD
D. William Moose, Jr., MD
Andrew G. Moran, MD
Rafael M. Moreschi, MD
Elena A. Morgan, MD
Michael C. Morin, MD
Constance Mulroy, MD, FACOG
Kalyan S. Muppavarapu, MD
Donald S. Murinson, MD
Anne P. Murphy, PA-C
Neill H. Musselwhite, III, MD
Benjamin J. K. Myers, DO
Kenneth W. Myers, MD
Praveen Namireddy, MD
Ali K. Nasim, MD
Wallace R. Nelms, Jr., MD
Kenneth E. Nelson, MD
Jonathan Nestor, MD
Pavlo I. Netrebko, MD, FACC
Paul C. Neuman, DO
Lanning R. Newell, MD
Justin V. M. Nguyen, MD
Franklin C. Niblock, IV, MD
Matilda W. Nicholas, MD, PhD
John C. Nicholson, MD
Stephen W. North, MD
Elizabeth I. Norton, PA-C
Andrew S. O'Connor, DO
Monica Oei, MD
Paul Y. Oh, MD
Matthew D. Olin, MD
Brian V. O'Neal, MD
Scott B. O'Neal, MD
Pamela S. Oravetz, PA-C
John W. Ormand, Jr., MD
Liston A. Orr, MD
Dinah H. Oxendine, PA-C
Aaron R. Pankiewicz, DO
Malcolm H. Pannill, II, PA
Alexander Paraschos, MD
Preeti H. Parekh, MD
H. Kim Park, MD
C. Lawrence Parker, MD
Shefali V. Parmar, MD
Vikas J. Patel, MD
Louie L. Patseavouras, MD
Rolvix H. Patterson, Jr., MD
Daniel E. Paul, MD
Stephanie O. Peacock, MD
David A. Pearson, MD
Martha G. Peck, MD
Suresh J. Penkar, MD
Rachel Peragallo Urrutia, MD
Bryan M. Peters, MD
Milan Petrovic, MD
Jerry M. Petty, MD
Eureka L. Phillip, MD
Aaron G. Pico, PA-C
Hubert G. Pierce, MD
Katherine J. Pierce, MD
Joseph A. Pino, MD
William G. Pittman, III, MD
Ivy P. Pointer, MD
Laura C. Politte, MD
Roberto C. Portela, MD
Benjamin P. Powell, MD
James B. Powell, MD
Thomas E. Powell, III, MD
Laura S. Pratt, PA-C
Dale P. Quirke, MD
Akef S. Rahman, MD
Natarajan Rajan, MD
Jitinder S. Rangar, MD
Jayalalitha Rao, MD
Anuradha Rao-Patel, MD
Inam Rashid, MD
Jennifer A. Ratley, DO
John M. Ray, Jr., MD
Lisa L. Ray, MD
Hannah Rayala
Leighton A. Raynor, MD
John B. Reckless, MD
Conor M. Regan, MD
Richard H. Reid, MD
William O. Renfroe, Jr., MD
Joel C. Reynolds, MD
Leslie D. Reynolds, MD
David L. Richardson, MD
David L. Riley, MD
Carlos M. Rish, MD
Richard S. Roberts, MD
Heather N. Robertson White, MD
Joseph J. Robinette, MD
Edward N. Robinson, Jr., MD, MPH
Lindsey M. Rose, MD
Laura B. Rosenzweig, MD
Bianca Rosso, MD
Matthew A. Rushing, MD
Richard W. Rutherford, Jr., MD
Michael W. Ryan, MD
Madeeha Saeed, MD, FACC
Hal D. Safrit, MD
Patrick J. Sammon, PA-C
James G. Scanlan, MD
Thomas V. Scarritt, Jr., MD
Deborah D. Schoenhoff, MD
John R. Schultz, MD
Jonathan E. Scott, MD
Tina L. Scott, PA-C
Matthew L. Segal, PA-C
Randolph P. Sellers, MD
Jacob P. Shaffer, MD
Shreena G. Shah, DO
Rajiv K. Sharma, MD
William A. Shearin, Sr., MD
John D. Shelburne, MD
Rakesh R. Sheliya, MD
Charles H. Shelton, III, MD
Vijay Sheshadri, MD
Patricia A. Shevlin, MD
Mark E. C. Shogry, MD
Naomi S. Simon, MD
Patrick J. Simpson, MD, FACC
Aliana P. Sindram-Trujillo, MD, PhD
Francis W. Slate, MBChB
Stanley F. Sliwinski, Jr., MD
Norman R. Sloop, MD
Cameron L. Smith, MD
Candace T. Smith, MD
David N. Smith, MD, FACP
Jennifer L. Smith, MD
Joshua D. Smith, MD
Lindsay N. Smith, PA-C
Peter K. Smith, MD
L. Paige Sokolsky, MD
Michael D. Sorensen, MD
Leo R. Spector, MD
Shirley H. Spedding, MD
Rachel L. Speicher, DO
C. Harrison Springfield, IV, MD
Tina E. Sprouse, MD
Andrew D. Staples, PA-C
Gregg J. Stashenko, MD
Svetlana A. Staub, MD
Scott T. Steffen, MD
Ryan A. Stephens, MD
Bryan S. Stonestreet, MD
Alan W. Story, MD
Nicholas E. Stratas, MD
Samuel A. Sue, Jr., MD
E. Amy Suttle, MD, FAAP
Katherine L. Swain, MD
Rosalea K. Taam-Akelman, MD
Carlos J. Tamayo, MD
Khalil S. Tanas, MD
John P. Tanner, MD
Wyndee B. Tarter, MD
William C. Tate, II, MD
James E. Taylor, II, MD
Gregory A. Tayrose, MD
Gregory P. Temas, MD
Su Wooi Teoh, MD
Andrea L. Terry, DO
Mohan C. Thakuri, MD
Devi Thangavelu, MD
Ashish D. Thekdi, MD
Kenneth C. Thompson, Jr., MD
Marvin W. Thompson, MD
Cecil K. Thoppil, MD
Kim M. Thorner, MD
Stephen T. Thuahnai, MD
Devin K. Tighe, MD
T. Keith Toledo, MD
Mary E. Tolle, PA-C
Sanjay Tomar, MD
Porshia M. Tomlin, MD
Ruben Torrealba, MD
Michael R. Towarnicky, MD
Murphy F. Townsend, Jr., MD
Lucas V. Tran, MD
Kelly E. Trawick, PA-C
Edward L. Treadwell, MD
Amanda C. Trimpey, MD, MPH, FACOEM
Gloria L. Tsan, MD
Wade R. Turlington, MD
W. Harrison Turner, III, MD
Benjamin D. Umbel, DO
Trevor C. Upham, MD
Martin Van Cleeff, MD
Joel D. VanderMey, PA-C
Michael V. Varricchio, Jr., PA-C
Muryel W. Vary, PA-C
Adrian Vazquez, MD
Jack L. Vesano, MD
Ashutosh R. Virmani, MD
Francis W. Wachter, MD
Deborah H. Waechter, MD
Analiese Wagner, DO
John E. Wahlen, MD
David A. Walker, MD
Lauren E. Wall, PA-C
Andrew B. Wallace, MD
Richard F. Walton, MD
William B. Warlick, Jr., MD
Julia G. Warren-Ulanch, MD
Zack J. Waters, Jr., MD
Jerry F. Watson, MD
Joseph S. Wehby, Jr., MD
Rodney D. Welling, MD
Timothy D. Wetzel, MD
Courtney M. Wharton, PA-C
Cynthia S. White, MD
Matthew S. White, MD
Paul C. Whitesides, Jr., MD
Allison C. Whitton, MD
Walter R. Whitworth, MD
Michael E. Wiegert, PA-C
Jeremy S. Wilkes, MD
Barton G. Williams, MD
David R. Williams, Sr., MD, FAAP
Dennis R. Williams, Jr., MD
Glenn E. Williams, PA-C
Mathew W. Williams, PA-C
Paul F. Williams, MD
Thomas R. Williams, MD
Deitra L. Williams-Toone, MD
L. Brent Wilshire, MD
Jack K. Wilson, Jr., MD
De Benjamin Winter, III, MD
Ryan J. Wise, MD
Jacob A. Wisniewski, MD
Jerry C. Woodard, MD
Paul R. Woodard, MD
W. Samuel Yancy, MD
Michael F. Yarborough, MD
Roger J. Yau, MD
Joshua C. Yelverton, MD
Alex G. Yip, MD
Hassan Yousaf, MD
Justin W. Zanone, MD
David P. Zarzar, MD



















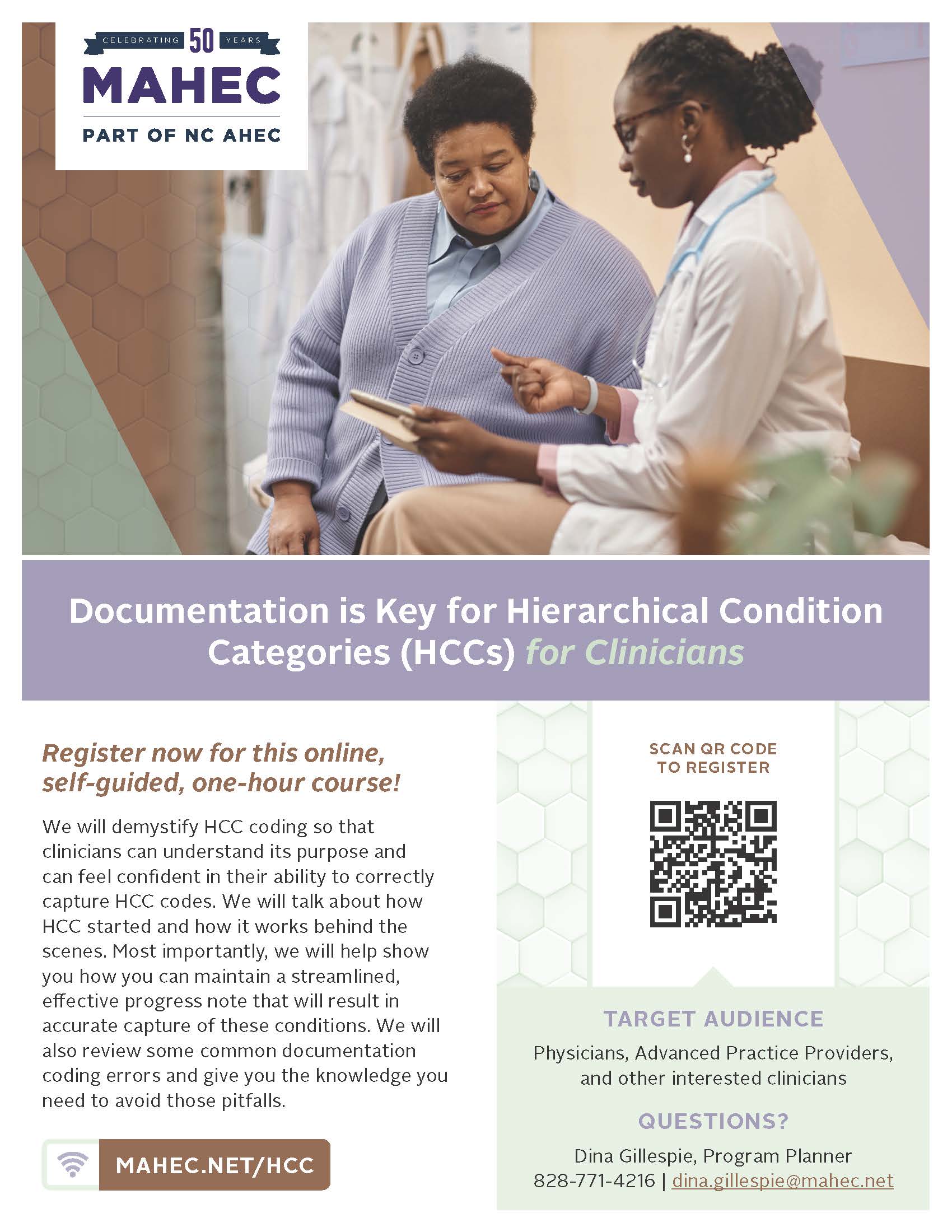
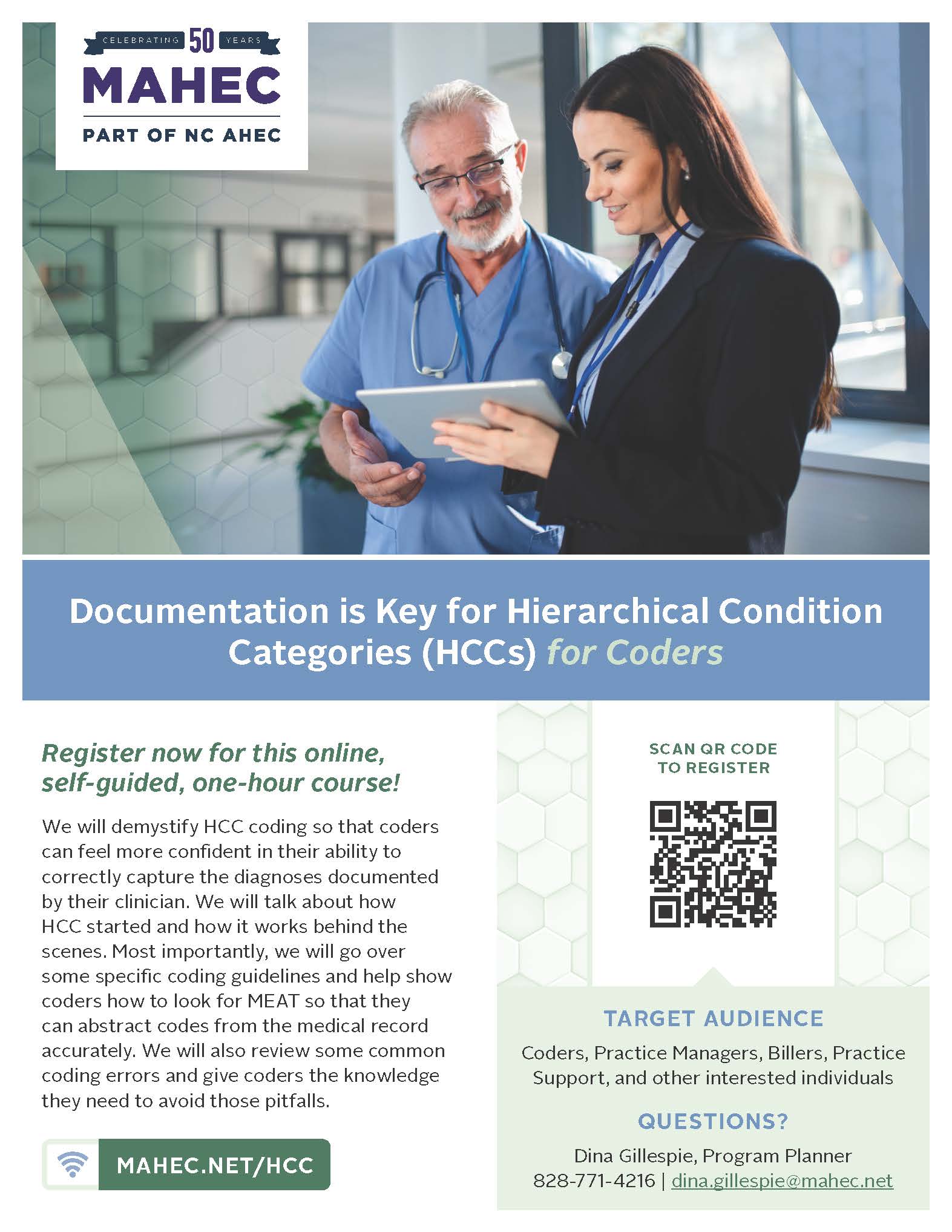















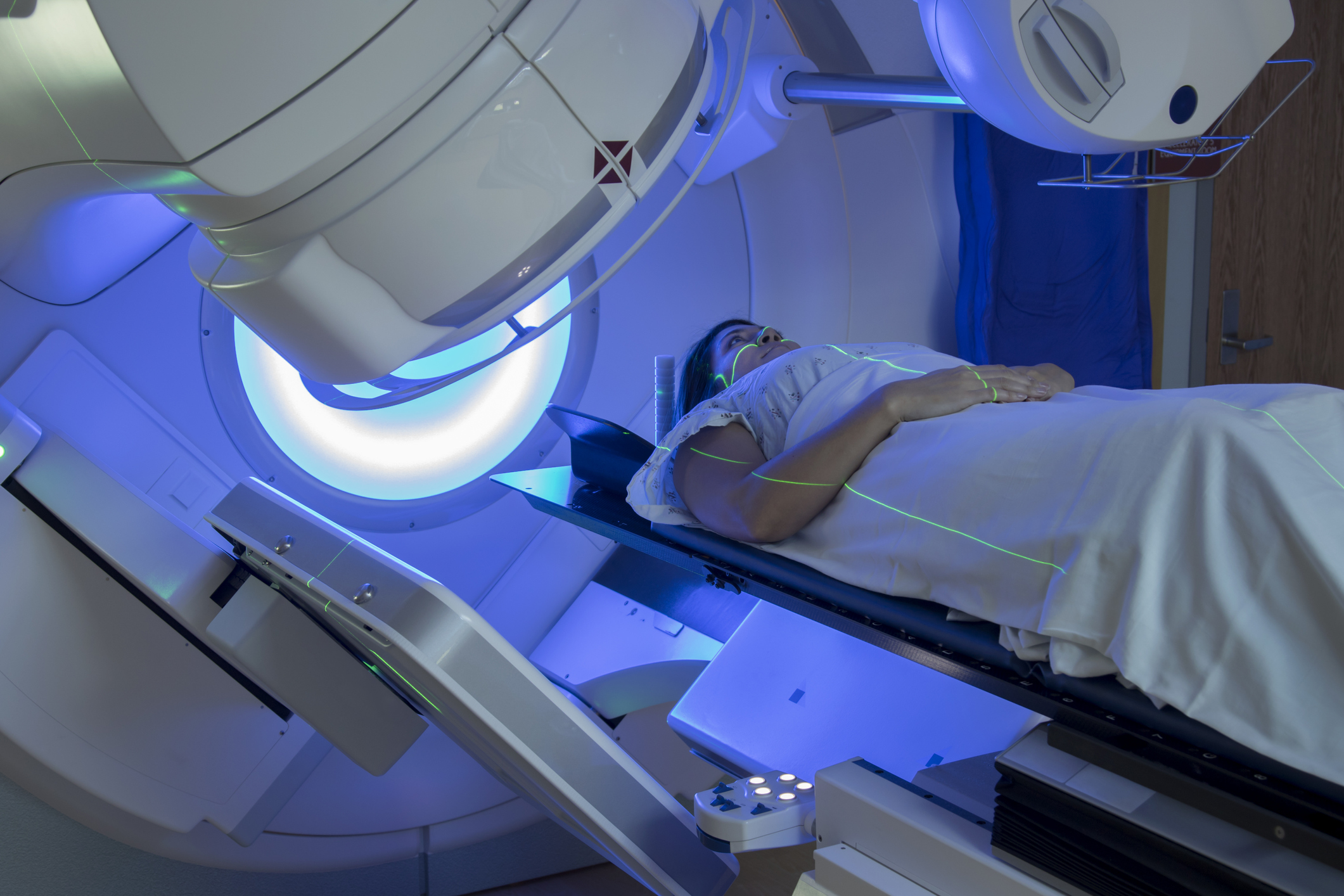
 [source]
[source]
















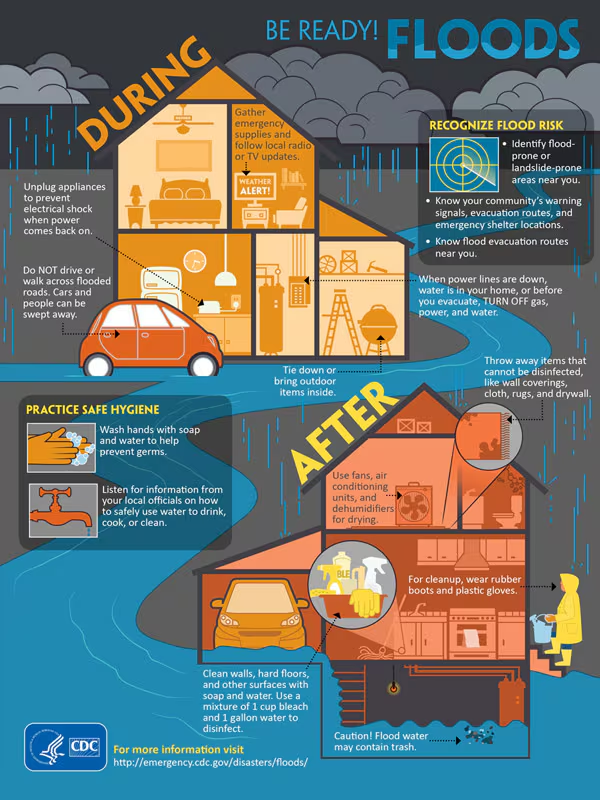 (image credit: CDC)
(image credit: CDC)









