
AMA Foundation Excellence in Medicine Awards Nominations NOW OPEN!
![]()
The AMA Foundation Excellence in Medicine Awards recognize physicians and medical advocates who exemplify the highest values of volunteerism, community engagement, leadership and dedication to the care of underserved populations. These awards highlight the critical role that physicians play and are intended to inspire others in and beyond the profession to strive for excellence.
Nominations for the 2024 Excellence in Medicine Awards are now open! Know an outstanding physician who goes above and beyond their everyday work? Nominate them today.
Awards will be presented during the AMA 2024 Annual Meeting in June.
For questions or additional information, contact Jennifer Leininger Knipstein, Senior Program Officer, AMA Foundation.
Deadline to nominate is February 5, 2024, at 11:59 p.m. CST.

HHS Improving Maternal Health Outcomes with New CMS Care Model

New Model Supports White House Blueprint on Maternal Health Crisis and CMS Action Plan
The U.S. Department of Health and Human Services (HHS), through the Centers for Medicare & Medicaid Services (CMS), announced innovative actions to improve maternal health and birth outcomes for pregnant and postpartum women and their infants through the new Transforming Maternal Health (TMaH) Model. This 10-year payment and care-delivery model will support participating state Medicaid agencies (SMAs) in developing and implementing a whole-person approach to pregnancy, childbirth, and postpartum care for women with Medicaid and Children's Health Insurance Program (CHIP) coverage. This model supports the White House Blueprint for Addressing the Maternal Health Crisis and the CMS Maternity Care Action Plan.
“The maternal health crisis in our country is unacceptable. The Biden-Harris Administration is committed to addressing this urgent issue and using all available means to eliminate disparities in our health care system,” said HHS Secretary Xavier Becerra. “This data-driven approach by CMS will help ensure we are improving outcomes for birthing parents and newborns. Expanding access to proven maternal health care best practices and initiatives will help moms and their children thrive.”
“CMS is taking a comprehensive, evidence-based approach to achieve our goal of making tangible improvements in maternal health and birth outcomes,” said CMS Administrator Chiquita Brooks-LaSure. “The Transforming Maternal Health Model furthers our commitment to improve the experience for all pregnant women across the country, regardless of their background and ethnicity.”
Despite spending more per capita for maternity care than any other nation in the world, the U.S. has higher rates of adverse pregnancy outcomes than any other high-income country. The goal of the TMaH Model is to ensure pregnant and postpartum mothers with Medicaid or CHIP health insurance receive personalized care that can improve their health outcomes, including fewer low-risk cesarean sections, and fewer instances of severe maternal morbidity. The TMaH Model also seeks to support or increase access to additional maternal care providers, such as midwives, birth centers, and doula services. Each participating state Medicaid agency will be eligible for up to $17 million during the model’s 10-year period.
"We have heard loud and clear that many women do not feel listened to or supported during their birth experience, and the current rate of maternal morbidity and mortality is deeply concerning,” said CMS Deputy Administrator and Innovation Center Director Liz Fowler. “This model aims to improve health outcomes for mothers and their newborns, and support a system that makes mothers feel empowered, safe, and healthy throughout their pregnancy and postpartum.”
To help mothers feel supported in their birthing plan, states participating in the TMaH Model will increase access to a variety of maternal health providers, such as midwives, freestanding birth centers, and doula services. Participating Medicaid agencies will work with their hospitals and health systems to help achieve the CMS “Birthing-Friendly” designation, which is the first federal quality designation with a focus on maternal health for hospitals and health systems. Additionally, states will foster connections to implement evidence-based practices and lessons, like monitoring pregnant women at home who are diagnosed with conditions that can lead to pregnancy-related complications, such as hypertension and gestational diabetes. Participating states will also have their maternity care providers screen for and address pregnant women’s health-related social needs – including, but not limited to, challenges like inadequate access to nutritious food, housing insecurity, or substance use disorder – by connecting mothers to community-based organizations.
Today’s announcement is the latest in a series of actions CMS is pursuing to further advance maternity care quality, safety, and equity. The Biden-Harris Administration has prioritized maternal health, including by urging all states and territories to provide a full year of continuous postpartum coverage through Medicaid and CHIP under the American Rescue Plan Act. To date, CMS has approved these postpartum coverage extensions in 40 states, plus Washington, D.C. and the Virgin Islands. In addition, the Administration deployed a “Birthing Friendly” designation icon on CMS’s Care Compare online tool to identify hospitals and health systems that participate in a statewide or national perinatal quality improvement collaborative program and that implement evidence-based care to improve maternal health — the first iteration of a federal quality designation with a focus on maternal health for hospitals and health systems.
For more detailed information about the TMaH Model, visit the model website: https://www.cms.gov/priorities/innovation/innovation-models/transforming-maternal-health-tmah-model
To read the TMaH Model Frequently Asked Questions, visit: https://www.cms.gov/tmah-model-frequently-asked-questions
For a fact sheet about the TMaH Model, visit: https://www.cms.gov/files/document/tmah-fs.pdf
Click here for the Journey Map: https://www.cms.gov/files/document/tmah-journey-map.pdf

Coming in January: NC Medicaid Point-of-Sale Vaccine Rate File

NC Medicaid maintains a Point-of-Sale (POS) vaccine rate file and will begin publishing the POS vaccine rate file on the Outpatient Pharmacy Services website under Reimbursement in January 2024. The POS vaccine rate file is based on NCPDP units and is updated as vaccines are added or discontinued for coverage in the POS setting.
NC Medicaid has been notified that NC Medicaid Managed Care plans may be reimbursing vaccine POS claims differently from the State. The NC Medicaid Managed Care plans are working to review their vaccine POS claims and reprocess. NC Medicaid reimburses vaccines at Wholesale Acquisition Cost (WAC) + 3% in the POS setting.
Currently, the NC Medicaid Managed Care plans may not cover all vaccines that NC Medicaid Direct covers at POS; however, beginning January 20, 2024, NC Medicaid Managed Care plans will begin covering vaccines at POS in the same manner as NC Medicaid Direct. In the interim, pharmacy providers should refer to communications from the beneficiaries’ plan for POS vaccine claim submission guidance.
- AmeriHealth Caritas North Carolina, Inc.
- Carolina Complete Health, Inc.
- Healthy Blue of North Carolina
- United Health Care of North Carolina, Inc.
- WellCare Health Plan
Based on updated CMS guidance related to the PREP Act, NC Medicaid will begin covering pharmacy POS claims for COVID-19 vaccines for beneficiaries ages 3 years and up through December 31, 2024, with an effective date of September 11, 2023. A revision is being made to the NC Medicaid COVID-19 Vaccine and Reimbursement Guidelines for 2023-2024 to reflect this as well.
As referenced in Vaccine Immunization Claims Can Be Submitted on Pharmacy Claims for NC Medicaid Direct Beneficiaries, In 2016, the Department of Public Health prohibited pharmacies from participating in the Vaccine for Children program, hence Medicaid only reimburses vaccinations by pharmacist immunizers to Medicaid beneficiaries 19 years of age and older (exception is made for COVID-19 vaccines as set forth by the 9th amendment to the PREP Act for the duration of its effect, also found in the Federal Emergency PREP Act).
Claims will deny if the beneficiary is less than 19 years of age unless the claim is pre-approved for pharmacy administration reimbursement OR if the vaccine administered is unapproved for administration by a pharmacy immunizer.
Two new COVID-19 vaccines were released and are now covered at POS with the effective date of November 13, 2023.
Additionally, NCTracks is working to reprocess claims for COVID-19 vaccines between September 11, 2023, and October 18, 2023, that did not pay the correct $65 administration fee for COVID-19 vaccines. No action is needed by providers to initiate the reprocessing. [source]

NC AHEC Seeking Proposals for Interprofessional Clinical Training Sites

The North Carolina Area Health Education Centers Program (NC AHEC) is seeking proposals to establish up to 5 rural interprofessional clinical training sites. Proposals must include how teaching sites will provide interprofessional training for medical students and nurse practitioner or physician assistant students to transform current models.
- Associated with House Bill 259 , Section 8.4 (a)
- Dates to Apply: 01/02/2024 (Request for Proposal will be released) – 02/16/2024
- Estimated Award Date: 03/01/2024
- Budget Maximum: $150,000 per teaching site/year. Award length will be two years with possibility of renewal for additional two-year periods, contingent on availability of funds and progress towards project goals.
Goal
The goal of this project is to establish model outpatient, team-based clinical teaching sites in rural North Carolina as part of a partnership with one or more medical student programs and at least one or more graduate nursing and/or physician assistant programs and with deliberate planning for interprofessional education and practice.
Who Can Apply
Community based primary care medical practices or groups of practices (Family Medicine, General Internal Medicine, General Pediatrics) in rural North Carolina are eligible to apply. Documented partnerships with North Carolina institutions that train medical students and nurse practitioner or physician assistant students (e.g., letter of support, academic affiliation agreement, etc.) is required.
Health Systems can submit one or more proposals to establish teaching sites. A site may have more than one location but will be considered one site for purposes of the proposal. Up to five sites will be funded in total.
More Information
An informational webinar will be held on January 5th, 2024 at 2:00 pm. Please register in advance to receive the link to connect: https://us06web.zoom.us/webinar/register/WN_35GBSPwSQj2vsCXPntAKAQ
Contact Us
Jill Forcina, RN, PhD: [email protected]
Adam Zolotor, MD: [email protected]

New Interactive Tools Aiming to Improve Health of North Carolinians with Prostate Cancer

The UNC Men’s Health Program and Carolina Demography have unveiled an interactive web-based tool aimed at raising awareness and addressing disparities related to prostate cancer in North Carolina.
The tool, “Prostate Cancer Across North Carolina,” provides a detailed, county-by-county map view of prostate cancer cases and deaths, offering valuable insights for local and state organizations as well as the public. The map helps users access downloadable county-specific prostate cancer reports utilizing the latest data from the National Cancer Institute’s State Cancer Profiles (currently from 2016-2020).
KEY FEATURES OF THE TOOL:
- County-by-County Map: The tool presents a visually compelling map of North Carolina, highlighting prostate cancer cases and deaths at the county level.
- Detailed Reports: Each county features a downloadable, detailed report, breaking down new cases and deaths by race/ethnicity, providing medical professionals, policy leaders and individuals a more complete as well as nuanced understanding of the prostate cancer landscape.
Read more about this initiative here.

NC Medicaid: Updated Requirements for Filling Prescriptions

Providers are encouraged to review an updated version of the following Medicaid Bulletin Article. The update includes links to the flyer and the beneficiary next steps document (also linked in the final paragraph of this bulletin) that the NC Medicaid team published to help inform members of the next steps:
- UPDATED: Requirements for Filling Prescriptions for Medicaid Beneficiaries: Reminder for the Expansion Population- NC Medicaid requires prescriptions to be ordered by Medicaid enrolled providers.
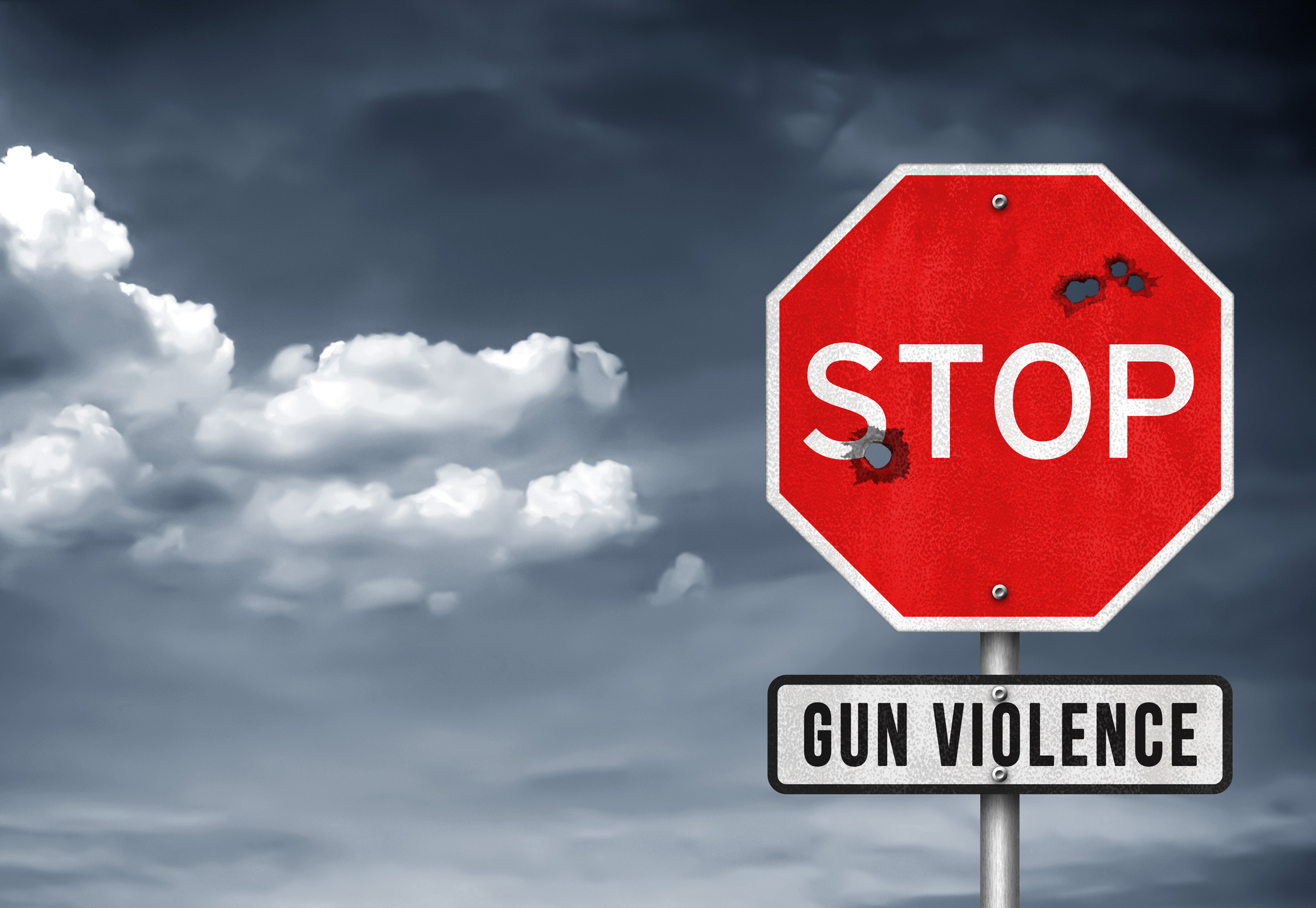
Hospital-based Violence Intervention Program Making Difference in NC

Last year, 393 gunshot wound victims, mostly men and juvenile males of color, were brought to the emergency department at Duke University Hospital.
Duke University Hospital launched the Duke Violence Recovery Program in September 2022 to support the needs of patients admitted to the Level 1 Trauma Center. Spurred by $375,000 from the federal American Rescue Plan, the hospital-based violence intervention program became the fifth of its kind in North Carolina, reframing violence as a preventable healthcare issue.
Led by Duke program manager Uzuri Holder and program coordinators Keith Patterson and Demetrius Lynn, the team supports residents in the city of Durham and Durham County who have experienced violence, with the goal of preventing readmission to the Duke Trauma Center.
Intensive case management starts in the emergency department with the patient and family members. Throughout a hospital stay, program staff meet with the patient and family.
“We’re a friendly face coming in and being helpful,” Patterson said. “Helping to get where they need to go, reassuring them and letting them know they have support inside the hospital.”
Team members follow residents between the ages of 15 and 40 for up to one year. During that time, case management support includes tackling concerns around housing, transportation, mental health, employment, life skills and more.
“The program is based on the premise of helping them complete the goals they set forth,” Holder said. “We want everyone to be healthy mentally, physically and accomplish everything they set forth and be in a space or place that is safest and healthiest for them.”
How the program makes a difference: In its first year, the Violence Recovery Program has engaged with roughly 160 patients, mostly gunshot wound victims. Program staff are a key part of the multidisciplinary team, bridging patients and caregivers.
The lived experiences of staff also help establish rapport.
In 1993, the program’s own Demetrius Lynn, a Durham native, survived a shooting in his hometown. At 20 years old, he was rushed to then-Durham Regional Hospital, where doctors saved his life.
During his three-month hospitalization, he underwent rigorous physical therapy. His family’s unwavering support and encouragement were vital in his recovery. Recognizing the importance of a strong support system, he now dedicates himself to assisting others through the program.
“Imagine being in a situation like that and you have no family support,” said Lynn, now 50. “You have no aspirations or hope of recovery. That’s when the program can come into play to fill the void.”
What’s ahead: Over the past summer, the program extended its services to include individuals who are victims of stabbings. The team aspires to broaden the program’s reach to encompass more programming.
“The next step is really to support all victims of violent crimes,” Holder said. “Right now, we’re at capacity for what we can handle, but that’s the goal.” [source]

NCTracks: Five New Exclusion Sanction Questions Added to Enrollment Applications in 2024

Beginning January 28, 2024, five new additional exclusion sanction questions will be added to enrollment, re-enrollment, full MCRs, office administrator (OA) and re-verification applications:
- L. Has the enrolling provider had any liability insurance carrier canceled, refused coverage, or rated up because of unusual risk or have any procedures been excluded from coverage?
- M. Has the enrolling provider ever practiced without liability coverage?
- N. Does the enrolling provider have any medical, chemical dependency or psychiatric conditions that might adversely affect your ability to practice medicine or surgery or to perform the essential functions of your position?
- O. Has the enrolling provider's hospital and/or Clinic privileges ever been limited, restricted, reduced, suspended, revoked, denied, not renewed, or have you voluntarily surrendered or limited your privileges during or under the threat of an investigation or are any such actions pending?
- P. Has the enrolling provider had a professional liability claim assessed against them in the past five years or are there any professional liability cases pending against them?
All five questions are applicable to individual providers. However; only two of the questions will be applicable to organizations:
- L. Has the enrolling provider had any liability insurance carrier canceled, refused coverage, or rated up because of unusual risk or have any procedures been excluded from coverage?
- M. Has the enrolling provider ever practiced without liability coverage?
Affirmative answers to exclusion sanction questions on all applications require a written explanation AND supporting documentation.
A thorough written explanation for each question answered affirmatively must be signed and dated by the responsible party within six months of the application date. Failure to disclose documentation related to an affirmative response will result in a denial of the application. A full explanation of the new documentation requirements can be found here.

Dosher Hospital in Southport to Host American Red Cross Blood Drive
Dosher Memorial Hospital is hosting an American Red Cross Blood Drive.

The event will take place on Friday, December 29th from 8:30am -1:30pm at the Jaycee Building, located at 309 N. Fodale Ave.
Community members who would like to donate blood are encouraged to sign up online at www.redcrossblood.org and enter in zip code 28461 in the “Find a Blood Drive” search tool. Look for the Jaycee Building on 12/29, and click, “See times,” to check schedule availability. Tap on the donation time of your choice and fill in the requested information. All donors are welcome. Please bring a photo ID.
Community members who have questions may call the Red Cross at 910-762-2683 or go to RedCrossBlood.org.

How You Can Improve Access for Medicaid Home- and Community-based Services

The U.S. Department of Health and Human Services (HHS), through the Centers for Medicare & Medicaid Services (CMS), today took another critical step to improve access to home-and community-based services (HCBS) by reminding states of tools to better connect direct support workers to individuals receiving Medicaid-covered HCBS, such as individuals with disabilities and older adults.
The agency’s new guidance focuses on building and maintaining worker registries — worker management platforms that make qualified health workers easier to find — so more individuals receiving Medicaid-covered services can receive care in a setting of their choice.
The guidance also notes significant federal funding available to help states build these registries thanks to President Biden’s American Rescue Plan (ARP).
Read the full CMS Press Release here.

New National Program Providing Free Telehealth Visits for COVID/Flu Patients

Under the new national Home Test to Treat Program, patients, regardless of insurance or immigration status, can get a free telehealth visit with a practitioner if they test positive for COVID or the flu. They can also get free or low-cost treatments (e.g., Paxlovid) delivered to their home or pharmacy. Also, all patients can once again get free COVID tests by mail.
The Home Test to Treat Program is funded by the National Institutes of Health (NIH) to better understand how technologies such as at-home tests and telemedicine can improve healthcare access for individuals across the country. Findings will be used to inform future public health programs for the American people. Any data shared with researchers will be limited to what is necessary to evaluate the program and will not include information which can identify individuals.
New Clinic Revolutionizes Cancer Care for Young Adults
“Be loud and explode with light, move with grace, have no fear.”

The UNC Adolescent and Young Adult Cancer Program, inspired by the dying wish of 15-year-old Sophie Steiner of Chapel Hill, is revolutionizing the supportive care of adolescents and young adults with cancer.
Opened in October by the UNC Lineberger Comprehensive Cancer Center, the Be Loud! Center for Young Adult Cancer Care is a new outpatient clinic for adults aged 18-39 on the third floor of the N.C. Basnight Cancer Hospital. The Be Loud! Sophie Foundation honors Steiner and a meaningful line she wrote before being stricken with a rare, aggressive and incurable form of cancer: “Be loud and explode with light, move with grace, have no fear.”
The inspiration
When Steiner was in the N.C. Children’s Hospital in 2013, she refused to let her cancer diagnosis define her. She still danced. She still laughed and made wisecracks. And she still cared about and loved people.
One day, when Steiner knew the final treatments were failing, she asked her parents Niklaus and Lucy Steiner for one last request in her obituary: to donate money to support adolescents and young adults facing cancer at UNC Hospitals.
Unexpectedly, tens of thousands of dollars poured in, and the Steiners – including Sophie’s siblings Elsa and Annabel – started the Be Loud! Sophie Foundation. The foundation, driven only by volunteers and with no paid staff, started raising money to bring about systemic change with the goal of funding a position at UNC Lineberger dedicated to addressing the unique needs of 13- to 39-year-old cancer patients.
With funding from the Be Loud! Sophie Foundation, Lineberger launched the UNC Adolescent and Young Adult Cancer Program and hired social worker Lauren Lux as program director in 2015. Since then, Be Loud! Lineberger, UNC Hospitals and other sources have raised enough money to increase the staff of one to a staff of 10 – and soon to be 11 – including medical director Dr. Andrew “Smitty” Smitherman, hired by Lineberger in 2017.
For the people, by the people
Jesse Sorrell, a former patient at UNC Hospitals, was 22 when he was diagnosed with melanoma in 2010. Sorrell’s treatment was successful, but in 2017 he was diagnosed with a progressive recurrence of stage-3 melanoma.
“My world flashed and crumbled before me,” Sorrell said at the dedication event for the clinic.
Sorrell co-created the UNC Adolescent and Young Adult Patient Advisory Board, an integral part of the design of the Be Loud! Center.
The center features a lounge and seven suites, each with a large chair for the patient and two seats for visitors. There are no televisions. Lights and dividers are adjustable. Windows are large to let light pour in, and blinds feature a tree design, as does the floor.
The space will feature rotating artwork by patients and caregivers. A framed guitar hangs on the wall, signed and donated by The Who’s Roger Daltrey and Pete Townsend, driving forces in the creation of Teen Cancer America.
“The crux of the issue and why we built this space is that teenagers and young adults can get lost in the healthcare system,” Lux said. “They’re not little kids and they’re not older adults. So it can feel like they are the only one their age going through what they are going through. This isolation is not a good feeling, and it isn’t necessary.” [source]

Don't Get Scrooged! Stay Alert Against this Growing Gift Card Scam!
Scammers are making the most wonderful time of the year complicated!

It's called card draining, and authorities nationwide are issuing a warning to those who have or plan to purchase gift cards this holiday season: exercise caution and look out for any signs of tampering, such as scuff marks or scratches near the bar code on the back of the card.
The card draining scam involves tampering with bar code on gift cards and stealing the money loaded on them. Here a few ways to protect yourself:
- Make sure the gift card is sealed and the protective cover and the tape covering the pin is intact
- Ensure the gift card does not appear to be tampered with
- Keep the store receipt in case the gift card you are purchasing is found to have been compromised
- If a purchased gift card is found to be compromised, immediately report it to the gift card company directly, to request a freeze on the card, and request a refund.
Read the full article here.

Join the CDC and AMA TOMORROW for Fireside Chat on Respiratory Virus Season

During the fall and winter, germs are more likely to spread within the community and within health care settings. As a health care professional, you play a critical role in slowing and preventing the spread of viral respiratory infections, including flu, COVID-19, and RSV. CDC’s Project Firstline can help you access the infection control information and resources you need to take action this respiratory virus season.
Join CDC and the AMA Tuesday, December 12, 1:45-2:30 p.m. ET, for a special fireside chat with CDC Director, Dr. Cohen, on how to protect yourself and your patients during the fall and winter respiratory virus season.
Register and submit your questions today.
Don’t miss the opportunity to hear from Dr. Mandy Cohen, Dr. Demetre Daskalakis, and Dr. Sandra Fryhofer as they discuss vaccinations and other tools that can keep everyone safe and healthy.


NCMS Capitol Chronicle - The No Fees for EFTs Act Introduced in Congress

Under the Affordable Care act of 2010, all insurers had to provide an electronic payment option. This provision created a new payor business model whereby insurers began to charge physicians’ practices a fee for electronic transfer of the funds they are owed.
Led by Congressman Greg Murphy, MD (NC-3), a bipartisan group of members of the US House of Representatives has introduced HR6487, the No Fees for EFTs Act. This bill would end an increasingly common, predatory practice: charging medical practices a fee to process electronic payments.
According to a report published by ProPublica, “insurers now routinely require doctors to kick back as much as 5% if they want to be paid electronically.”

"Fees associated with electronic transactions for physician services are an unnecessary and costly burden on providers and patients," said Dr. Murphy in a press release on the bill. "We don't tolerate paying fees to receive direct deposit of a paycheck, likewise, doctors and patients should not be forced to pay predatory fees on electronic payments on essential health services."
The bill has gained bipartisan support in the House and we will continue to follow its progress.
Do you know your state and federal legislators?
More importantly, do your legislators know you?
The NCMS can help you connect with policy makers as a constituent and advocate!


Deadline Extended! More Time for Physicians Foundation Leadership Award Program
The Physicians Foundation has extended its call for nominations for the Leadership Award Program! New or early-career physicians are now encouraged to apply by January 31, 2024.
![]()
The Physicians Foundation’s Leadership Awards Program recognizes physicians for extraordinary actions in their practice or community. Award recipients will receive a $10,000 scholarship to elevate their efforts to address drivers of health (DOH) or advance innovative solutions to make their communities or practices a healthier place for patients and physicians.
Nominations will fall into two award categories:
- The Dr. Buz Cooper Award for Addressing Drivers of Health: In alignment with the Foundation’s work to recognize and act on challenges related to DOH, this award honors a physician who has gone above and beyond to connect their patients with the social, economic, educational and environmental resources that they need for their overall health. The award’s namesake is Richard (Buz) Cooper, MD, author of Poverty and the Myths of Health Care Reform.
- Medical Innovator Award: The Physicians Foundation champions the role of physicians as stewards for high-quality, cost-efficient care. The Medical Innovator Award recognizes a physician who has innovated and successfully implemented a new solution to strengthen the physician-patient relationship, support their medical practice’s sustainability or navigate the changing health care system.
Requirements include:
- Open to physicians who are new or early-career (practicing less than 15 years).
- Demonstrate physician leadership in relevant award category.
- Be nominated by a sponsor (mentor, colleague or peer) in coordination with the nominee. Sponsors should provide a short statement of recommendation.
- Submit a video component, current resume/CV and a statement that briefly describes how the scholarship will allow them to continue making positive, constructive contributions to the medical profession.

About The Physicians Foundation
The Physicians Foundation is a nonprofit seeking to advance the work of practicing physicians and help them facilitate the delivery of high-quality health care to patients. As the U.S. health care system continues to evolve, The Physicians Foundation is steadfast in strengthening the physician-patient relationship, supporting medical practices’ sustainability and helping physicians navigate the changing health care system. The Physicians Foundation pursues its mission through research, education and innovative grant making that improves physician wellbeing, strengthens physician leadership, addresses drivers of health and lifts physician perspectives. For more information, visit www.physiciansfoundation.org

NC Spine Society Call for Abstracts. Submit Yours Today!
Mark your calendars for June 7-9, 2024 for the NC Spine Society's next Annual Meeting at the Benton Convention Center in Winston-Salem, NC!

The North Carolina Spine Society is seeking scientific papers and abstract submissions from members, fellows and residents-in-training interested in participating in the program. If you have presented to the Society in the past few years, you are encouraged to present a follow-up on your research or long-term study results.
Please complete this Lecture Abstract Form to submit your entry by the response deadline of Friday, December 15. If you are selected to present, you will be required to complete and submit a Conflict of Interest Disclosure form for CME purposes.
U.S. Set to Approve First Gene-editing Treatment for Sickle Cell Patients
U.S. regulators are expected to approve exa-cel for use in sickle cell patients by the end of this week. The U.K. approved it under the brand name Casgevy last month.
Regulators in the U.S. are also reviewing another gene therapy from Bluebird Bio called lovo-cel. It works differently than exa-cel but is administered similarly and is also intended to eliminate pain crises. It's expected to be approved later this month.
Approval of exa-cel by the U.S. Food and Drug Administration would mark a scientific milestone about a decade after the discovery of CRISPR and a breakthrough for patients desperate for a better option.
Read more on what is happening here.
Related reading:
Gene Therapy for Sickle Cell Disease Approved in UK. What Could this Mean for US?
New Advancements Could Make Cure for Sickle Cell Disease a Reality
ECU Health Sets Focus on Sickle Cell Research

NC Study Awarded $21 Million to Reduce Inequities in Maternal Health Outcomes

A study between the UNC Chapel-Hill and Orange County Health Department, called “Thriving Hearts: Healing-Centered, Integrated, Community Maternity Care,” has been approved for a $21-million funding award from the Patient-Centered Outcomes Research Institute (PCORI), an independent, nonprofit organization based in Washington, D.C. The funding award will be used to reduce the incidence of hypertensive disorders of pregnancy (HDP) and improve maternal outcomes across 10 North Carolina counties over the next six years.
In the United States, rates of maternal mortality and severe maternal morbidity are rising, especially among Black and American Indian/Alaska Native women and women with disabilities, low incomes, or rural residences. Black women with HDP - a group of high blood pressure disorders that includes preeclampsia and gestational hypertension - are 3.7 times more likely to die from complications and are more likely to experience severe morbidity than their white counterparts.
The project, led by Alison Stuebe, MD, professor of obstetrics and gynecology at the UNC School of Medicine, and Quintana Stewart, director of Orange County’s Health Department, will be coordinating with local health departments, families, and community groups to make pregnancy and birth safer. Their project strategy involves a multi-level intervention to provide support and connection at the individual patient level, the healthcare team level, and the community level.
“The overarching goal of ‘Thriving Hearts’ is to cultivate conditions for mothers to not only survive pregnancy, but to thrive,” said Stuebe, who is also a Distinguished Scholar of Infant and Young Child Feeding at UNC Gillings School of Global Public Health. “By implementing a multi-level intervention, we want to help community advocates, health system leaders, and policymakers understand what types of support matter to growing families.”
Dr. Stuebe is a member of the NC Obstetrical and Gynecological Society, managed by the North Carolina Medical Society.
Read the full article here.
Great News for Your Patients! They May Be Eligible for Health Care Coverage through NC Medicaid.
NC Medicaid now covers people ages 19 through 64 years with higher incomes. Your patients may be able to get health care coverage through Medicaid even if they did not qualify before. NC Medicaid pays for doctor visits, yearly check-ups, emergency care, dental care, mental health and more – at little or no cost to recipients.
Most people can get health care coverage through NC Medicaid if:
- You live in North Carolina
- You are ages 19 through 64 years old
- You are a citizen (some non-US citizens can also get health care coverage through Medicaid).
And if household income falls within the chart below:
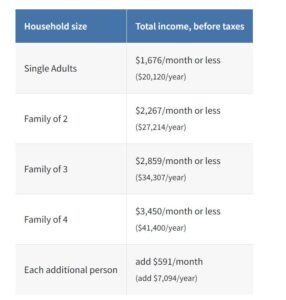
If someone is pregnant, they may be eligible for other Medicaid programs to get full health benefits.
NC Medicaid covers most health services. It includes doctor visits, check-ups, emergency care, hospital services, maternity and postpartum care, vision and hearing services, prescription drugs, behavioral health, preventive and wellness services, dental care, medical-related devices and more. There is no monthly fee and copays are never more than $4.
Learn how to apply here.
For Questions and Answers about Medicaid Expansion, click here.
Resources clinicians may find helpful:
- Download a one-page flyer explaining Medicaid services and who is eligible.
- Download a one-page flyer explaining the new coverage available to participants in the Family Planning Medicaid program.
- View a short PowerPoint deck that can be used to explain Medicaid expansion to your community.
NCTracks Reminder: Provider Name on Applications Must Match for Re-verification
The provider name listed on applications for re-verification must match their legal name, name on the National Plan and Provider Enumeration System (NPPES) Registry, and their name on any license, certification, and/or accreditation.
Providers can check their listed NPPES name at: https://npiregistry.cms.hhs.gov/search
If the name does not match, do NOT submit the application. Instead send an email to [email protected] with required documentation attached.
See chart on this page for more information about required documentation.
NCMS PAC Thankful Thursday!
On this Thankful Thursday, we are recognizing some of our NCMS PAC Investors! Thank you for your continued investment in your patients and profession. Contact Hannah Rice ([email protected]) to learn more about how you can make a difference.
Cynthia J. H. Brown, MD
Daniel H. Nguyen, MD
Edward N. Robinson, Jr., MD, MPH
John A. Thomas, MD
Mary Ann Contogiannis, MD
Sanjay Tomar, MD

From the Bottom of Our Hearts, THANK YOU!

On behalf of the NCMS Foundation, we want to say THANK YOU to those who participated in #GIVINGTUESDAY!
Thanks to your generosity, this year was one of the BEST ever!
Together we are helping to improve the health and wellbeing of North Carolinians.
Learn more about the NCMS Foundation here.


Register Now! AMA Advocacy Insights Webinar: Strategies to Address the Nation’s Worsening Drug Overdose and Death Epidemic

Registration is open for the next webinar in the AMA Advocacy Insights series – “Strategies to address the nation’s worsening drug overdose and death epidemic” – on December 12 at 11:30 a.m. Central time.
The 2023 AMA Overdose Epidemic Report finds that – despite positive actions from physicians, growth in harm reduction services, and policy advancements – the nation’s drug overdose and death epidemic is deadlier than ever. The annual report details many of the reasons the epidemic persists, largely due to illicitly manufactured fentanyl and the continued lack of meaningful implementation and enforcement of policies that support affordable, accessible, and evidence-based care for patients with substance use disorders or pain.
Learn more in this webinar about policy actions that need to be taken, harm reduction strategies that should be implemented more broadly, and efforts by physicians and the AMA Substance Use and Pain Care Task Force to end the epidemic.


EXTENDED! More Time to Meet Making Care Primary Application Deadline
DEADLINE EXTENDED!
The Centers for Medicare & Medicaid Services (CMS) has announced a new voluntary value-based primary care model called Making Care Primary (MCP). With a planned launch date of July 1, 2024 in eight states, including North Carolina.
The 10.5-year model aims to improve care management and care coordination, equip primary care clinicians with tools to form partnerships with health care specialists, and leverage community-based connections to address patients’ health needs.
CMS is now accepting non-binding applications from Medicare-enrolled organizations that provide primary care services to fee-for-service Medicare beneficiaries. The application deadline is December 14, 2023.
NC AHEC has developed an MCP playbook for potential applicants, which contains concepts about the MCP model and its design, timelines, evaluation tools, considerations, and resources. It's a must-see for those interested in applying!
For more information, visit CMS here.

Medicaid Expansion Could Help North Carolina's Overdose Crisis
NCDHHS says that between 2000 and 2022, more than 36,000 North Carolinians lost their lives to drug overdose.

There could be some relief coming to rural areas in North Carolina that continue to deal with the opioid crisis. Better treatment options are some of the benefits of Medicaid expansion, according to Kody Kinsley, the secretary of the state’s Department of Health and Human Services.
Kinsley described overdose losses as “deaths of despair” — saying they often occur when people are struggling with mental illness, lack social connection or have a negative life event such as a job loss.
He says many people who could not get treatment in the past will now be able to do so through the Medicaid expansion that began last week. He says with the right care and support, they can reconnect with those around them.
“They're working again, they're taking care of their families, they're paying taxes, they're supporting their rural communities and they're making it vibrant,” he says.
Kinsley says there’s another benefit to getting rural residents with drug addictions medical help under Medicaid: it will take a burden off local law enforcement. [source]

20 NC Hospitals Receive High Honors for Maternity Care
More than 20 North Carolina hospitals were rated among the best regional hospitals for maternity care, according to U.S. News and World Report.
On Tuesday, the publication released its list of the best hospitals for maternity care for uncomplicated pregnancies.
UNC Hospitals in Chapel Hill, UNC Rex Hospital in Raleigh, WakeMed Hospital in Cary and Raleigh and Duke Regional Hospital in Durham were all named high-performing in maternity care.
North Carolina hospitals that were named high-performing for maternity care for uncomplicated pregnancies:
- Alamance Regional Medical Center
- Atrium Health-Cabarrus
- Atrium Health-Pineville
- Atrium Health-University City
- Catawba Valley Medical Center
- Duke Regional Hospital
- Moses H. Cone Memorial Hospital
- Novant Health Forsyth Medical Center
- Novant Health Huntersville Medical Center
- Novant Health Matthews Medical Center
- Novant Health New Hanover Regional Medical Center
- Novant Health Presbyterian Medical Center
- Novant Health Thomasville Medical Center
- UNC Hospitals
- UNC Rex Hospital
- WakeMed Cary Hospital
- WakeMed Raleigh Campus
“Hospitals that receive a High Performing designation as part of Best Hospitals for Maternity Care meet a high standard in caring for parents with uncomplicated pregnancies,” said Jennifer Winston, Ph.D., health data scientist at U.S. News. “These hospitals have C-section rates that are 26% lower, and newborn complication rates that are 37% lower than unrecognized hospitals that participated in the survey. Parents-to-be can research their local hospitals’ performance metrics for free at health.usnews.com to help them choose where to have their baby.” [source]

Join DOCMS' Final Meeting of the Year
Join DOCMS at the University Club!
Wednesday, December 13, 2023 | 6:00pm - 8:00pm
University Club, 3100 Tower Boulevard, Suite 1700 - Durham, NC 27707
AGENDA:
- 6:00pm- 6:30pm – Socializing & Housekeeping
- 6:30pm- 7:30pm – Dinner & Guest Speaker
- 7:30pm- 7:45pm – Q&A
- 7:45pm- 8:00pm – DOCMS 2023 Business
REGISTER NOW - Hybrid Meeting
"Burnout; why is the intensity of the flame worsening, despite increasing research and awareness?"
Dr. Damian McHugh

A two-way discussion about “why is the data-do gap getting worse”. We have known about burnout for 40+ years, so why is it now critical in medicine – and law, in our military, animal vets and teachers?
This article will be a nice compliment to the discussion.
Dr. Damian McHugh bio:
Proud father of two hungry teens, eager (but still poor) golfer, husband of Marion – trauma nurse turned travel nurse consultant, I graduated Med School in 1990 at Manchester UK. Having become a member of the Royal College of GPs, I swerved specialties and changed countries. Having repeated a full EM Residency at UNC, I spent 21 wonderful years at the Rex ER in Raleigh.
Since ending my clinical practice, I've been afforded the privilege of walking the back 9 of my career as SVP Physician Liaison at Curi, a full-service physician advisory firm headquartered in Raleigh. Each day that I wake, I'm driven to discover how better our company (which is owned by its 14,000+ member physicians) can make their lives better in Medicine, Business and Life.
I'm passionate about burnout, having seen so many colleagues brought to their knees by a complex medical system that so often appears to place dollars ahead of patients and their providers.
REGISTER NOW - Hybrid Meeting
Questions or can you not open the registration google link?
Please email Frank Snyder at [email protected]
1 CME Credit is available! Click here for how to claim your credit.
DOCMS Members & Prospective Members - FREE to attend
Guests - $25 to attend (will be collected at meeting site)
A Zoom link will be sent to registered attendees on August 9th.

NCTracks December Provider Training Schedule Now Available

Registration is open for the December 2023 instructor-led provider training courses. NCTracks Zoom courses can be attended remotely from any location with a computer and internet connection. Individualized meeting information has been created for each course.
Courses include:
- Submitting a Professional Claim- Provider NEMT
- New Office Administrator
- Recipient Eligibility Verification
- Prior Approval Medical
- Submitting Professional Claims
- Dental Helpful Hints
Please see the Course Information and Training Enrollment Instruction details here.

NCMS Leadership College Alum Named President of NCAFP
NCMS member and Leadership College Alum Dr. Garett Franklin named President of the North Carolina Academy of Family Physicians.

Dr. Garrett Franklin, a native of Drexel, NC, is the new president of the North Carolina Academy of Family Physicians. He attended North Carolina State University graduating with a BS in engineering in 2003, a BA in chemistry in 2007 and a Masters of Physiology in 2008. He completed medical school at the Brody School of Medicine at East Carolina University in 2012 and went on to complete his family medicine residency and a primary care sports medicine fellowship at Wake Forest Baptist Medical Center.
Franklin became involved in the NCAFP’s advocacy efforts as a resident at Wake Forest and has served on the Board of Directors for the last five years. He practices family medicine and sports medicine at Raleigh Medical Group/Cary Medical Group in Raleigh, while also working at NC State University as a team physician. He is active in academic and clinical research and many advocacy projects.
Franklin and his wife have a son and daughter and live in Raleigh. He has been a member of the North Carolina Medical Society since 2008.

NC DHHS Launches New Performance Dashboard for 988 Suicide and Crisis Lifeline

The North Carolina Department of Health and Human Services has launched a performance dashboard for the 988 Suicide and Crisis Lifeline to highlight how the suicide and crisis lifeline is being used in North Carolina.
The 988 Suicide and Crisis Lifeline connects North Carolinas via call, chat or text to a trained crisis counselor who will listen, offer support and provide community resources 24 hours a day, 7 days a week. 988 is a state-federal partnership between NCDHHS and the U.S. Substance Abuse and Mental Health Service Administration. It was implemented nationwide in July of 2022.
"North Carolina is a national leader in operationalizing 988 which is a critical part of the state's crisis system," said NC Health and Human Services Secretary Kody H. Kinsley. "With shortened response times and more connections made, 988 is a powerful tool in helping to get North Carolinians the support and resources they need when they need them."
The dashboard shows North Carolina is successfully meeting demand for the 988 service. North Carolina outperforms national averages in several key areas. For example, it takes 14 seconds to answer calls in North Carolina whereas the national average is 39 seconds. North Carolina also answers 98% of all calls received, compared to the national average of 90%. And the dashboard indicates a 25% increase in utilization over the past year, which shows the service is playing a valuable role for North Carolinians in need of mental health resources.
The 988 performance dashboard provides useful information on contact volume, answer rates, speed of answer, age ranges and reasons for calling. It also indicates call volume for specific populations, including North Carolinians who reach out to the Spanish call center, Veterans Crisis Line and the LGBTQ+ youth and young adult line (e.g., the Trevor Project Line). Data shared in the dashboard does not include personal or confidential health information.
"Understanding how this service is being used and by whom are keys to understanding where our crisis system is working well and where it needs to be improved," said Kelly Crosbie, MSW, LCSW, Director of the NCDHHS Division of Mental Health, Developmental Disabilities, and Substance Use Services. "The 988 dashboard will help us build the accountability necessary to ensure people get care they need when and where they need it."
988 is an important component of our overall crisis system. The new state budget invests $131 million to expand and strengthen crisis services in North Carolina. In addition to 988, several key community-based crisis services are funded, such as:
- Mobile Crisis Teams: Immediate, on-site support for people experiencing a mental health and/or substance use crisis
- Facility-Based Crisis Centers and Drop-in Centers: Community-based crisis centers for individuals experiencing a behavioral health or substance use crisis
- Non-Law Enforcement Pilot Program: Transportation services to psychiatric facilities that do not involve law enforcement
- Behavioral Health (BH) SCAN: Statewide bed registry that helps hospitals and other providers facilitate and track referrals and access to inpatient, crisis, residential and community levels of care
The department is currently developing its implementation plan for these investments and is keeping people informed through a monthly webinar titled "Side By Side." It is hosted by the Division of Mental Health, Developmental Disabilities, and Substance Use Services. For more information, or to register as an attendee for one of these webinars, please visit the Side By Side meeting registration link.
988 is available to anyone, anytime. If you or someone you know is struggling or in crisis, help is available. Call or text 988 or chat 988lifeline.org. Individuals who speak Spanish can now connect directly to Spanish-speaking crisis counselors by calling 988 and pressing option 2, texting "AYUDA" to 988, or chatting online at 988lineadevida.org or 988Lifeline.org.
Prescription Reimbursement Change for Non-Medicaid Enrolled Providers
Medicaid expansion launched on December 1, 2023, and NC Medicaid is reminding providers that prescriptions written by non-Medicaid enrolled providers will not be reimbursable by NC Medicaid due to federal requirements. NC Medicaid requires that all providers whose NPI will be used on a pharmacy claim be enrolled with NC Medicaid. There are no exceptions to this requirement. This bulletin applies to NC Medicaid Direct and NC Managed Care.
NC Medicaid anticipates close to 300,000 new beneficiaries will receive full Medicaid coverage through Medicaid expansion on Dec. 1, 2023. Many of these beneficiaries may have had primary care services in free and charitable clinics who do not bill and are not enrolled in NC Medicaid.
- This means that beneficiaries with prescriptions from non-Medicaid enrolled individual providers will be denied coverage, and the beneficiary will not be able to fill their prescription through the NC Medicaid benefit.
- The pharmacy may fill the prescription at full cost for the beneficiary.
For clinics that dispense medications at no cost to patients, providers should consider dispensing an additional 30-day supply of medications to support the new Medicaid beneficiary during the transition period to allow time for beneficiaries to engage with their new NC Medicaid provider and/or time for non-Medicaid providers to enroll in NC Medicaid. Non-enrolled providers are encouraged to consider enrolling in NC Medicaid so prescriptions can be covered benefits.
To receive payment for office visits for Medicaid beneficiaries, a provider must fully enroll; however, there is a “lite” enrollment option that will allow providers to enroll as an Ordering, Prescribing, Referring (OPR) provider.
- The OPR provider enrollment process is a simpler and easier path to enroll into NC Medicaid only for the purposes of ordering, prescribing and/or referring beneficiaries for services.
- The estimated completion time for OPR provider enrollment is approximately one to two weeks from the application submission (if there are no issues with the submitted application).
- Enrolling as an OPR only provider would enable providers to prescribe medications, which are billed to NC Medicaid by the pharmacy, without the provider having to enroll as a full rendering Medicaid provider.
- If a provider would like to continue to serve NC Medicaid beneficiaries, providers must enroll as a full Medicaid provider.
Non-Medicaid enrolled providers treating beneficiaries who will enroll in NC Medicaid through Medicaid expansion should submit an OPR application as soon as possible. To enroll in NC Medicaid as an OPR only provider, providers can go to the NCTracks Provider Enrollment page.
- Under Quick Links, there is a user guide for “How to Enroll in NC Medicaid as an Individual Practitioner.”
- Select “Ordering, Prescribing, Referring Providers Enrolled with the Lite Application” (or if fully enrolling, select “Individual Full Enrollment”) as the Provider Enrollment Application Type.
- After submitting the application, applying providers should make sure to quickly respond to any notification regarding the application and reach out for assistance as soon as needed to ensure quick resolution of any open items impacting enrollment.
For more information on OPR provider enrollment, please review the OPR Provider FAQs.
When pharmacies process prescriptions for NC Medicaid beneficiaries that are denied due to the provider not being enrolled, pharmacists should encourage beneficiaries to schedule an appointment with their new NC Medicaid enrolled provider as soon as possible.
Beneficiaries should also be encouraged to seek out urgent care, Federally Qualified Health Centers (FQHCs) or the emergency department if they have an immediate need for medications to avoid gaps in care. Additionally, if the beneficiary received a prescription from a free clinic, the beneficiary should be encouraged to go back to the free clinic to refill their prescription until they are able to set-up an appointment with their NC Medicaid provider. Pharmacists are also encouraged to reach out to non-Medicaid enrolled providers regarding enrollment and to inquire if there is another NC Medicaid provider with an established relationship with the beneficiary who can write a new prescription for the beneficiary.
In summary, please see the below actions for prescribers and pharmacies:
1. Actions for Prescribers: Non-Medicaid enrolled providers treating a beneficiary enrolling in NC Medicaid through Medicaid expansion should consider applying to enroll in NC Medicaid. No additional action is needed for actively participating providers.
- To receive payment for office visits for Medicaid beneficiaries, a provider must fully enroll in NC Medicaid.
- If the only intent is to ensure prescriptions are paid by Medicaid, non-enrolled providers may choose the lite enrollment option which only allows claim payment when the provider is ordering or referring for services or prescribing medications. The lite provider enrollment process is a simpler and quicker way to enroll into NC Medicaid when the provider does not intend to bill for rendered services.
2. Actions for Pharmacies: When pharmacies process prescriptions for NC Medicaid beneficiaries, which deny due to the provider not being enrolled, they should:
- Contact non-Medicaid enrolled providers regarding enrollment and to inquire if there is another NC Medicaid provider with an established relationship with the beneficiary who can write a new prescription for the beneficiary.
- Encourage beneficiaries to schedule an appointment with their new NC Medicaid enrolled provider as soon as possible.
- Encourage beneficiaries to seek out urgent care or the emergency department if they have an immediate need for medications or a medical emergency.
- Encourage beneficiaries to go back to the free clinic (if applicable) to refill their prescription until they are able to set-up an appointment with their NC Medicaid provider.
For questions, contact NCTracks Call Center: 800-688-6696

Register Now for Improving Child and Youth Mental Health Webinar Happening Tomorrow

The Improving Child and Youth Mental Health: Driving Factors and Root Causes webinar will highlight the report, Addressing the Long-Term Effects of the COVID-19 Pandemic on Children and Families (2023).
Drawing on the work of the Board on Children, Youth, and Families in the Division of Behavioral and Social Sciences and Education and the Health and Medicine Division at the National Academies of Science, Engineering, and Medicine, this webinar will focus on the driving factors that contribute to the children and youth mental health crisis, including disparities and inequities in the mental health system.
Speakers will include:
- Leslie Walker-Harding, Division Chief and Director Ford/Morgan Endowed Professor and Chair, Seattle Children's Hospital (Moderator)
- Margarita Alegria, Professor, Departments of Medicine & Psychiatry, Harvard Medical School, Chief, Disparities Research Unit, Department of Medicine, Massachusetts General Hospital, Harry G. Lehnert, Jr. and Lucille F. Cyr Endowed Chair, Mass General Research Institute, Massachusetts General Hospital
- Tumaini Rucker Coker, Professor and Division Head of General Pediatrics, University of Washington School of Medicine, and Seattle Children’s Hospital
- Kimberly E. Hoagwood, Cathy and Stephen Graham Professor of Child and Adolescent Psychiatry, New York University Langone Health
- Caren Howard, Senior Director, Policy and Advocacy, Mental Health America

Happy Birthday to These NCMS Members Celebrating This Month!
Grab your party hats and noisemakers and let’s celebrate!
Randy S. Adams, MD
Swati S. Adawadkar, MD
Briggs M. Ahearn, MD
Collette Ah-Tye, MD
Edward S. Alessandrini, DMD, MD
Richard J. Alioto, MD
E. Jackson Allison, Jr., MD, MPH
Simon J. Allport, MD
Barry D. Amos, MD
Swathi B. Anche, MD
Sarah M. Anderson, MD
Wallace F. Andrew, Jr., MD
Bradley L. Anglemyer, MD
William E. Anthony, Jr., MD
Andrew P. Apicella, PA-C
Gregory C. Appert, MD
Ana M. Arango, MD
Perico N. C. Arcedo, III, DO
Dina L. Arceo, MD
Louis C. Argenta, MD
Tracy O. Arusuraire, MD
Nancy J. Astle, MD
Savana E. Atkins, PA
Sam T. Auringer, MD
T. James Baden, MD, FACP
Charles E. Baker, MD
Vansanth B. Baliga, MD
Charles L. Baltimore, Jr., MD
W. Byron Barber, II, MD
Joseph U. Barker, MD
Christopher J. Barnes, MD
Laura A. Barton, PA-C
Laura B. Barton, PA-C
Karen L. Bash, MD
Tara K. Bastek, MD
Sanjay Batish, MD
Gregory S. Bauer, MD
Margaret R. Beal, PA-C, MMS
V. Edward Bean, MD
L. Neal Beard, Jr., MD
Walter B. Beaver, Jr., MD
Gregory G. Bebb, MD
Michelle L. Beckham, MD
Timothy M. Beittel, MD
James E. Bellard, MD
Barbara A. Bergdolt, MD
Donald R. Bergsma, Jr., MD
Chudaratna Bhargava, MD
Edgardo H. Bianchi, MD
Karl F. Bitter, MD
James F. Black, MD
Jesse A. Blackman, MD
Susan Blackwell-Crawford, PA-C
Benjamin R. Blaschke, PA-C
Seth J. Bleier, MD
Charles J. Blevins, MD
Robert J. Board, MD
Edwyn T. Bowen, Jr., MD
James H. Bradford, MD
Genevieve N. Brauning, MD
Karen E. Breach Washington, MD
Katherine L. Breiter, MD
Samuel E. Britt, II, MD
M. Todd Brown, MD
Natalie Bruce, MD
George F. Brumback, MD
Tracie C. Bryson, MD
Joseph A. Buglisi, Jr., DO
Kerry C. Bullerdick, MD
Nicole P. Bullock, MD
Richard A. Bunio, MD
Holly J. Burge, MD
Rollin S. Burhans, Jr., MD
J. P. Burnette, MD, FACP
Brandon C. Burnsed, MD
D. Scott Burton, MD
Jeffrey W. Byrnett, MD
Marco A. Caceres, MD, FACS
T. Francis Camp, Jr., MD
Leah A. Carlson, MD
Kevin W. Carroll, MD
Fred A. Caruso, MD
Venkata R. Challa, MD
H. Royster Chamblee, Jr., MD
Jeffery A. Chance, PA-C
E. Ted Chandler, MD
Ku-Lang Chang, MD
Benjamin C. Chasnis, DO
Abdul G. Chaudhry, MD, FACS
Nicole R. Check, MD
Peter G. Chikes, MD, FACS
Terry C. Childers, MD, FAAP
Stephanie M. Chismar, DO
Stephen K. Chiu, MD
San H. Choi, MD
Windy D. Christy, PA-C
Derek Clar, DO
Erika L. Clark-Trapp, MD
Shelby L. Clay-Rogers, MD
Richard B. Clinton, MD
Bruce E. Cohen, MD
James B. Collawn, MD
Filiberto Colon, II, MD
Jessica S. Connett, MD
Tim E. Cooper, Jr., MD
Charles I. Cooperberg, MD
Anureet C. Copeland, MD
A. James Coppridge, MD
Asa L. Cordle, MD
Joseph B. Cornett, MD
Benjamin B. Covell, MD
Chad E. Cox, MD
Karen L. Cross, MD
James J. Crossley, MD
John T. Curnes, MD
John W. Currens, MD
Mark A. Curzan, MD
Samuel J. Dail, MD
Liam N. Daly, MD
Aaron P. Danison, DO
Uma U. Darji, MD
Marc A. Darst, MD
David A. Dasher, MD
Andrew Davidson, MD
Kevin R. Davidson, MD
D. Whitaker Davis, MD
Devon L. Davis, MD
Robin L. Dawson, PA-C
Ernesto E. de la Torre, MD
Patricia Y. De Tomas-Medina, PA-C
James P. Deering, III, MD
John O. delCharco, MD
Jessica C. Derreberry, MD
Christopher F. Dibble, MD
Edward E. Dickerson, IV, MD
Ellen D. Dillavou, MD
Michael J. Donahue, MD, FAAD
Venkatarama S. Donepudi, MD
Kristin L. Donoghue, MD
Kevin E. Dougherty, MD
Ryan C. Dougherty, MD
Caron L. Dover, MD
Carrie A. Dow-Smith, MD
Laurel L. Drayton, PA-C
Melora T. Driver, MD
Vincent J. D'Souza, MD
Frederick M. Dula, Jr., MD
Raymond B. Dyer, MD
Matthew D. Dyson, MD
J. William Eakins, MD
R. Crews Edens, PA-C
Kim D. Edhegard, II, MD
Lorven M. Edralin, MD
Amanda E. Edwards, PA-C
Charles D. Edwards, MD
Stephen P. Ellison, MD
Miles Elmore, MD
John A. Engelmann, Jr., MD
Nathaniel Erskine, MD
Joseph J. Estwanik, MD
Anna F. Fakadej, MD
Ann E. Farash, MD
Bruce E. Fee, MD
Dale E. Feldpausch, Jr., MD
Ana C. G. Felix, MD
Juan B. Firnhaber, MD
David M. Fisher, MD
Lara L. Fisher, MD
Kellie E. Flock, PA-C
Rajat R. Fofaria, MD, FACC
Richard S. Foulke, MD
James J. Foutty, MD
Casey N. Fox-Morea, PA-C
Nicholas Frankel, MD
Mel W. Fryar, MD
Kiana M. Fussner, PA
Walter H. Gajewski, MD
P. Mark Gallerani, MD
Gabryel L. Garcia-Sampson, MD
Lars B. Gardner, DO
W. Ronald Gardner, MD
Edgar C. Garrabrant, III, MD
James E. Garrett, MD, FACEP
Joshua E. Garriga, MD
Scott K. Garrison, MD
Cynthia M. Gary, PA-C, MPH
Byron M. Geer, DO
Ashley L. Gelinas, MD
Henry Gerock, MD
Martin T. Gessner, MD
Robert W. Gibson, MD
Charles D. Godwin, MD
Geraldine F. Goertzen, MD
Manuel J. Gorrin-Rivas, MD, PhD
James A. Graham, MD
James J. Green, Jr., MD
P. David Green, MD
Kimberly M. Greenwald, MD
Kathryn M. Greven, MD, FASTRO
Andrew S. Griffin, II, MD
Joe W. Grisham, MD
Christopher T. Grubb, MD
Cesar Guajardo, MD
W. Bonner Guilford, MD
Ashraf F. Guirgues, MD
Jagmohan D. Gupta, MD
Khie S. Ha, MD
Michel G. Haddad, MD
M. Suzanne Hampson, MD
Aaisha S. Haque, MD
Kyle C. Harner, MD
Charles D. Harr, MD
Phillip G. Harris, MD
Samuel R. Harris, MD
Joseph S. Healy, MD
Jessica A. Hedrick, PA-C
Scott A. Hees, DO
Steven M. Heffner, MD
Craig S. Heinly, MD
William R. Henrick, MD
Richard C. Herring, MD, MBA
Heath C. High, MD
Philip L. Hillsman, MD
Kiem M. Hioe, MD
Angela S. Hira, DO
Jonathan N. Ho, MD
Mary K. Hoffman, MD
Carla W. Holder, MD
Christopher M. Holland, MD
Michael D. Holland, MD
Walter B. Holland, MD
Steven D. Hollosi, DO
John D. Holly, MD
Kenneth A. Holt, MD
W. Borden Hooks, III, MD, FACS
Jennifer J. Hoover, MD
Teague L. Horton, MD
Frank M. Houston, MD
Joshua L. Hudgens, MD
Alese V. Hunt, MD
James A. Hunter, MD
Joseph T. Inglefield, III, MD
Thomas G. Irons, MD
Hicham S. Ismail, MD
Mark T. Jackson, MD, FAAP
Ashok Jain, MD, MBA, FAAP
Francis M. James, III, MD
Edward O. Janosko, II, MD, FACS
Jennifer A. Jarosz, MD
S. Taylor Jarrell, MD
Robert G. Jeffers, MD, MPH, FAAP
Robert B. Jennings, MD
Rupert W. Jilcott, III, MD
Suresh Jillellamudi, MD
Carrie E. Johnson, MD
Delores L. Johnson, MD, FACOG
Matrika D. Johnson, MD
Ryan C. Johnson, MD
John D. Johnston, MD
William O. Jolly, III, MD
Enrico G. Jones, MD
James D. Jones, MD
Jason D. Jones, MD
J. W. Jones, MD, FACP, AGAF
Allen M. Joseph, MD
Ismo M. Kaariainen, MD
Jacob A. Kahn, MD
Scott M. Kahn, MD
Haku K. Kahoano, MD
David M. Kaplan, MD
Christina M. Karr, PA-C
Sanjeev Katyal, MD
Douglas G. Kelling, Jr., MD, FACP
Jeffrey S. Kelly, MD
William H. Kelly, MD
Kirsten S. Kerr, MD
Christine M. Khandelwal, DO
Gautam Khandelwal, MD
Khalid W. Khayr, MD
George R. Kilpatrick, Jr., MD
Whitney L. Kirchoff, MD
Richard E. Kleinmann, MD
J. Douglas Knoop, MD
Lawrence H. Knott, Jr., MD, FACS
William G. Kodzai, Jr., MD
Sarath C. Kolluru, MD
Shawn D. Kosnik, DO
Paul J. Kostuchenko, MD, PhD
William H. Kouri, MD
Kevin L. Krasinski, MD
Jack J. Kuritzky, MD
Cameron J. Kurowski, MD
Ryan P. Lamb, MD
Graham G. Lashley, MD
Mark K. LaVigne, MD
Marley B. Lawrence, MD
David L. Leader, Jr., DO
Tami A. Lee, PA-C
William D. Lee, Jr., MD
Gail A. Leget, MD
Nancy C. Lehman, MD
Eric J. Lescault, DO
Daniel R. Lewis, MD
Jonathan L. Lin, MD
Kanhka Linthavong, MD
Peter M. Lipscomb, MD
Jennifer Lira, MD
Allison K. Little, PA-C
Charles W. Lomax, MD
Otis M. Lowry, MD
L.D.A. C. Luvis, MD, FACP
Yvonne Luyando, MD
William D. Lyday, MD
Kimberly G. Lykins, DO
Nchimunya M. Maambo, PA
Henry J. MacDonald, Jr., MD
Mary T. MacKenzie, MD
Jerome J. Magolan, Jr., MD
Ureena Manandhar, MD
Wissam B. Mansour, MD
R. Wade Markham, MD
James W. Markworth, MD
Bernard A. Marshall, MD
Dennis L. Martin, MD
Tiffany Marum, MD
Jordan S. Masters, MD
Michael J. Masters, MD
Emmett C. Mathews, Jr., MD, FACC, FACP, FAHA
Kimberly R. Maurer, MD
A. Thomas May, III, MD
Ronald B. May, MD, FAAP
David B. Maybee, MD
David W. McAllister, MD
Jane H. McCaleb, MD
Chad M. McCall, MD, PhD
Robert J. McCammon, MD
Keith L. McCormick, MD
Kimberly A. McCrea, MD, FCCP
John T. McElveen, Jr., MD
Damian F. McHugh, MD, FACEP
Anjanette L. Mcilwain-McCollum, MD, FAAP
Karin R. McLelland, MD
Julian E. C. McLeod, PA-C
Steven J. McMahon, MD
John T. McMurtry, MD
Wendy W. McNeill, MD
Victor A. Medina, MD
Joan N. Meehan, MD
Milap P. Mehta, MD
John J. Meier, IV, MD
Frank M. Melvin, MD
Roman G. Melvin, MD
H. Curtiss Merrick, MD, FACP
David F. Michael, MD
J. Lloyd Michener, MD
R. Alden Milam, IV, MD
Edith H. Miller, MD
Maxwell S. Miller, DO
Sarah J. Mills, MD
Megan E. Milne, MD
Americo M. Minotti, MD
C. Brent Mizelle, MD
Linda C. Mohr, MD
Gregory J. Mohs, MD
John L. Monroe, MD
Robert W. Monteiro, MD
Daniel H. Moore, MD, FACOG
Alan L. Morgan, MD
Robert G. Morgan, Jr., MD
Jacqueline H. Morris, DO
Artus M. Moser, Jr., MD
Amir R. T. Motameni, MD
Jon Mugweru, MD
Joseph L. Murad, MD
Daniel W. Murphy, MD
Katherine A. Murphy, PA-C
Kelly R. Murphy, MD
Mark T. Murphy, MD, FACC
Richard J. Murphy, MD
Sean J. Murphy, DO
Joanna D. Murray, PA
Holly C. Musgrove, MD
Matthew B. Myers, MD
Keith V. A. Nance, MD
Myra Flor Nario, PA-C
Rushi K. Nayak, MD
Charles R. Neal, MD
William A. Nebel, MD
David S. Nelson, MD
Edwin C. Newman, III, MD
Rosemarie C. Newman, MD, FACOG
Gregory S. Nichols, DO
Peter J. Noone, MD
Mary C. Notaro, DO
Charles F. O'Cain, MD
Michael J. O'Connell, DO
Brian P. O'Donnell, MD, FAAP
Ambrose S. Okonkwo, MD
John G. Oliver, MD
Michael R. Oswald, MD
Harold P. Overcash, MD, FAAP
Carroll C. Overton, MD
Alexander T. Page, MD
Branson H. Page, MD
Hannah M. Palko, PA-C
John A. Papalas, III, MD
Kenneth S. Papier, DO
Pankaj N. Parikh, MD, FACC
Danna M. Park, MD, FAAP
Eunee K. Park, MD
Robert I. Park, MD
Danielle E. Parrish, PA-C
James S. Parsons, MD
Amish V. Patel, MD
Beena N. Patel, DO
Sanjay A. Patel, MD
William R. Patton, MD
Alfredo L. Pauca, MD
Matthew W. Payne, MD
James V. Perciaccante, MD
Jasper B. Perdue, Jr., MD
Henry T. Perkins, Jr., MD
Paul C. Perlik, MD
Everett L. Perry, MD
Jennifer H. Peterson, MD
Noel Peterson, MD
Frederick E. Pfeiffer, MD
Linda C. Pham, PA-C
Dana P. Piasecki, MD
Noah R. Pierson, MD
Harold C. Pillsbury, III, MD, FACS
Holly T. Pilson, MD
Joseph K. Piscitello, MD
Stuart W. Point, MD
Denise Poland-Torres, PA-C
A. Shaye Polk, PA-C
Stewart M. Polsky, MD
William L. Pomeroy, III, MD
Matthew A. Popa, MD
James R. Post, MD
James B. Powell, II, MD
Kothai Divya Pragatheeshwar, MD
James E. Pugh, Jr., MD
Amitabh Purohit, MD
Shrinivas Rajagopalan, MD, PhD
Jennifer L. Raley, MD
R. Pinkney Rankin, Jr., MD
Michael P. Ransone, MD
Tayyabah Rayyast, PA-C
Kelsey L. Rea, PA-C
Kelly K. Redden, DO
Lloyd F. Redick, MD
F. Ed Reedy, Jr., MD, FAAP
Steven H. Reid, MD
Caroline E. Reinke, MD
Donald P. Renaldo, MD
Christopher R. Reynolds, MD, FACEP
Jonathan C. Riboh, MD
Anne S. Richardson, MD
Michael A. Richman, MD
Scott C. Rissmiller, MD
Jesse E. Roberts, MD
Leroy Roberts, Jr., MD, FACR
Stephen C. Robinson, MD
Shannon M. Roche, DO
R. Mark Rodger, MD
David H. Rosenbaum, MD
Michael D. Rosenberg, MD
Elizabeth G. Rossitch, MD
R. Kyle Rothman, MD
Michael C. Rowland, MD
Alethea Y. Rucker, MD
Kathleen R. Ruddiman, DO
Roberto Rupcich, MD
Jarmella P. Russell, MD
Jeffrey K. Russell, MD
William J. Rutledge, MD
Philip R. Saba, MD
Barbara E. Salamon, MD
David L. Saliba, II, MD
M. A. Samia, MD
James R. Sancrant, Jr., DO
Daniel R. Scanga, MD
Charles W. Scarantino, MD, PhD
Richard J. Schneider, MD
Lisa C. Scott, MD
E. James Sebold, MD
Ashish P. Shah, MD
Christopher T. Shah, MD
Hadley J. Sharp, MD
Traci E. Sheaffer, MD
Steffany B. Shearer, DO
Mary D. Shearin, MD
Robert E. Shepherd, MD
Richard H. Shereff, MD
Roger D. Shetterly, MD
Frank W. Shields, IV, MD
Wright D. Shields, MD
J. Daniel Shoffner, MD
Steven A. Siciliano, MD
Leah M. Sieren, MD
David W. Sillmon, MD
Marshall A. Silverman, MD, FACP
Wendy W. Simmons, PA-C
Douglas K. Slater, MD
Andrew J. Smith, MD
David L. Smith, MD
Heatherly M. Smith, PA-C
Henry L. Smith, II, MD
Ian M. Smith, PA-C
S. Keith Smith, MD
Timothy T. Smith, DO
T. Truett Smith, Jr., MPAS, PA-C
Mona M. Soliman, MD
Jessica Son, MD
David R. Sopko, MD
Stephen C. Sorsby, MD
Gwyneth A. Spaeder, MD
Tiffany M. St. Clair, MD
Carey V. Stabler, MD
Walter J. Steele, MD
William R. Stetler, Jr., MD
Amanda R. Steventon, MD
William L. Stewart, MD, FAAP
Christopher A. Stiff, MD
Russell B. Stokes, MD
Michael W. Stratemeier, MD
Christopher T. Stuart, MD
Geeta Subramaniam, MD
Slade A. Suchecki, DO
Jeffrey M. Suchniak, MD
Sang H. Suh, MD
Chasity N. Sullivan, PA-C
Emily X. Sun, MD
Yun Sun, MD
Shane M. Sundlie, MD
Blythe W. Swaim, PA-C
Jason A. Swenson, MD
Bradley M. Swinson, MD
Danielle M. Sykes, PA-C
Shan Tang, MD
Robert B. Tannehill, MD
Muhammad F. Tariq, MD
Eli C. Tate, MD
Barry H. Teasley, MD
Teresa N. Terezis, MD
Alan R. Thalinger, MD
Chanchamma A. Thannikkary, MD
Brian T. Theune, MD
Christopher C. Thomas, MD
David T. Thomas, MD
Alan M. Thomley, MD, FACC
R. Morris Treadway, Jr., MD
Robert C. Turner, MD, FACP
James W. Turpin, MD, MPH
Maria G. Uberti, MD
Jamie Udwadia, MD
Chinazor O. Umerah, MD, MBA, FACP
Ryan C. Vann, PA-C, MHS
Daniel P. Vaughan, MD
William B. Veazey, MD
Ralph N. Vick, MD
Nicholas A. Viens, MD
Keith E. Volmar, MD
Kerri M. Wahl, MD
Aikya F. Waldo, MD
William R. Walker, MD
Kelley Wallace, Jr., MD
Peter A. Wallenborn, III, MD
Stephen L. Wallenhaupt, MD
Yi-Zhe Wang, MD
Patrick L. Ware, MD
John G. Warren, PA-C
Nikunj P. Wasudev, MD
James M. Watson, MD
Polly J. Watson, MD
Samantha S. Watson, MD
Stanley R. Watson, MD
John A. Watts, V, MD
James P. Weaver, MD
Andrew B. Weber, MD
Jade E. Weeks Kimble, PA-C
Michael D. Wehmueller, MD
Jack H. Welch, MD
John A. Welshofer, MD
David R. Wiercisiewski, MD
William D. Wilcox, MD
Geoffrey E. Wile, MD
Robert F. Wilfong, MD
Margaret J. Willhide, MD
Catherine E. Williams, PA-C
Christine A. Williams, PA-C
Martin K. Williams, MD
Noelle L. Williams, MD
Adam K. Willson, MD
Charles F. Willson, MD
Heber G. Winfield, III, MD
Christopher E. Winstead-Derlega, MD
Robert I. Wodecki, MD
Michael R. Wolff, MD
Neil T. Wolfman, MD
Sharon A. Wolters, MD
Jonathan Wons, MD
Terri A. Wood-Cummings, MD
Charles T. Woodham, MD, FACS
Richard H. Wray, III, MD
Thomas H. Wroth, MD
Lawrence R. Wu, MD
Jesse G. Yarborough, Jr., MD
Stephen M. Yeh, MD
Daniel M. Yoder, MD
Judith S. Yongue, MD
Sung-Eun Yoo, MD
Robert K. Yowell, MD
Mark S. Zalaznik, MD
Juozas A. Zavadzkas, MD
Deborah F. Zimmermann, PA-C
NC DHHS to Host RSV, Syphilis, Electronic Birth Registration Webinar
![]()
NC DHHS/Division of Public Health, in collaboration with NC AHEC, will be hosting a webinar on Monday, December 4, at 6pm, to provide updates on:
- The launch of new electronic birth registration system
- Congenital syphilis in North Carolina
- RSV vaccination during pregnancy
More information is available at here.
Online registration is available here.
Please share this information with interested colleagues.
![]()

Medicaid Redetermination – Physicians Survey

The North Carolina Medical Society has been asked to assist the Center for Medicare & Medicaid Services in ensuring Medicaid patients maintain coverage during the Medicaid redetermination period. CMS is interested in physicians’ experiences in particular.
North Carolina physician feedback would be helpful, and we would be grateful if you would respond to a survey to share your experience and insights. Please reply by Tuesday, December 5th.
Survey questions include:
- What Medicaid unwinding policies/strategies are working well? What is not working well?
- What barriers/ challenges have you faced during the unwinding?
- Are you/your practice working directly with patients to help them maintain Medicaid coverage or to transition to another form of coverage?
- Are you/your practice working with our state’s Medicaid managed care plans (Prepaid Health Plans / PHPs) or other private insurers to help connect patients with coverage options?
If so, what strategies are working well?
- What would be helpful to assist you and your practice in navigating the unwinding and assisting patients with maintaining coverage?
Please feel free to share this notice and survey link with your colleagues.
Thank you for your assistance. Your feedback (excluding your name and contact information) will be shared with CMS.
Secure Your Spot at the NCMS Advocacy Summit!
You're Invited to the NCMS Advocacy Summit!
This groundbreaking event is dedicated to exploring and advancing crucial topics in healthcare. Join us on March 23, 2024, from 9 am to 5 pm at the McKimmon Center, 1101 Gorman Street, Raleigh, NC 27606.
Don't miss this opportunity to be part of a transformative event. Secure your spot today by registering!
Registration is Open! Space is Limited!
NCMS PAC Thankful Thursday!
On this Thankful Thursday, we are recognizing some of our NCMS PAC Investors! Thank you for your continued investment in your patients and profession. Contact Hannah Rice ([email protected]) to learn more about how you can make a difference.
Ashley McKinney, PA-C
Christoph R. Diasio, MD, FAAP
David B. Eddleman, MD
Domenic A. Palagruto, II, DO
James C. Johnson, MD
Marian E. Cranford, PA-C
Shawn Parker

It's Giving Tuesday! Give North Carolinians Access to Care This Year!

During the next 24-hours, people around the world will come together to live out philanthropy – love of humanity – by giving to important causes.
The NCMS Foundation’s important cause is one we suspect is near to your heart too – ACCESS TO CARE.
The Foundation’s piece of this complex puzzle is providing financial incentives and practice support to primary care and behavioral health MDs, PAs and other clinicians as incentive to work in areas of NC that lack sufficient health care professionals and services.
With your help, we can make sure that ALL North Carolinians have an equal chance at healthy lives.
Thank you in advance for your support of the NCMS Foundation!


Polysubstance Abuse Worsening US Opioid Crisis

America's addiction crisis is being ushered into a dangerous new era by rising levels of polysubstance abuse, as more people become addicted to deadly combinations of synthetic opioids and stimulants. The alarming trend is causing concern among addiction specialists and medical professionals, who say the rise of polysubstance abuse is making it harder to treat opioid addiction and taking the crisis to a new, more perilous level.
What is polysubstance abuse?
Polysubstance abuse is described by the U.S. Centers for Disease Control and Prevention (CDC) as the "use of more than one drug." This includes when multiple drugs are taken at the same time or "within a short time period," the CDC explained, "either intentionally or unintentionally." When done intentionally, polysubstance use typically occurs when someone "takes a drug to increase or decrease the effects of a different drug or wants to experience the effects of the combination," the CDC added. Unintentional use happens when someone unknowingly takes drugs that were cut or mixed with other drugs. Either way, the consequences can be deadly because the effects from a combination of drugs "may be stronger and more unpredictable than one drug alone."
Mixing substances is never safe, but combining drugs from opposite drug classes can be especially deadly. Contrary to what some substance users believe, mixing stimulants and depressants "doesn’t balance or cancel them out," the CDC said. "In fact, the results of combining drugs are unpredictable, often modifying or even masking the effects of one or both drugs." This could create the illusion that "the drugs are not affecting you, making it easier to overdose," the agency added.
Continue to the full article here.
Feel the Joy of Giving Back Tomorrow During #GivingTuesday!
Don’t forget to share the love with others on #GivingTuesday!
Tomorrow, as people around the world support important causes, donate to the NCMS Foundation to provide access to NC’s uninsured and under-insured patients.
Your gift will help bring primary care and behavior health MDs, PAs, and other clinicians to mostly rural areas of the state that lack sufficient medical professionals and services, making sure ALL North Carolinians have an equal chance at healthy lives.
Join us in tackling this cause and spread the word to friends and family who also want to make an impact.
Get ready, this #GivingTuesday is going to be a wonderful way to kick off the season of giving!

Energy Assistance Program Helps Older North Carolinians with Heating Costs
![]()
The North Carolina Department of Health and Human Services' Low Income Energy Assistance Program will begin accepting applications from older adults and people with disabilities on December 1, 2023.
The federally funded program helps low-income households with a one-time payment sent directly to their heating vendor to offset the high cost of warming their homes during the cold weather months.
"We know the cost of most things are increasing, and keeping homes warm and safe this winter will be a bigger burden for some of our neighbors," said Carla West, Senior Director for Human Services at NCDHHS. "LIEAP helps ensure North Carolina's older adults and people with disabilities who may be facing a financial hardship have the funds to help stay warm throughout these colder months."
Payments will be distributed automatically to heating vendors beginning in December 2023 if a member of the household meets the following three requirements:
- Is age 60 or older or a person with a disability receiving services through the NCDHHS Division of Aging and Adult Services,
- Currently receives Food and Nutrition Services and
- Received a LIEAP payment during the 2022-2023 season.
Households meeting the requirements for the automatic payment will be notified of their eligibility in November 2023 and do not need to re-apply for LIEAP.
Any household with a person 60 or older or with a disability and is receiving services through the Division of Aging and Adult Services who did not receive notice of an automated payment, can apply online at epass.nc.gov. Applicants can also call their county department of social services to apply by phone, in person or print a paper application from epass.nc.gov to mail, fax or drop off at their county department of social services.
To be eligible for the LIEAP program, a household must:
- Have at least one U.S. citizen or non-citizen who meets the eligibility requirements,
- Have income equal to or less than 130% of the federal poverty limit, and
- Be responsible for their heating cost.
Beginning January 2, 2024, all other eligible households who meet the eligibility requirements may begin applying. Applications will be accepted from January 2, 2024, to March 31, 2024, or until funds are exhausted.
Last year, the LIEAP program provided approximately $63 million to help more than 143,000 households pay their heating bills from December 2022 through March 2023. For more information on the program and eligibility, visit here.

New Tribal Affiliation for American Indians on Birth and Death Certificates in NC
![]()
The North Carolina Department of Health and Human Services is taking steps to modify the representation of tribal affiliation on birth and death certificates.
"The department is committed to presenting the accurate representation of all people on vital records," said NCDHHS Chief Health Equity Officer and Deputy Secretary for Health Equity, Debra Farrington. "We appreciate the collaborative efforts with the American Indian community and the North Carolina Commission on Indian Affairs to develop these changes to birth and death certificates."
Effective August 28, 2023, all death certificates registered or amended in the North Carolina Database Application for Vital Events (NCDAVE) Electronic Death Registration System and issued by NCDHHS Office of Vital Records include the following race and tribal affiliation options for decedents who identified as American Indian:
- American Indian
- American Indian – Coharie
- American Indian – Eastern Band of Cherokee Indians
- American Indian – Haliwa-Saponi
- American Indian – Lumbee
- American Indian – Meherrin
- American Indian – Waccamaw-Siouan
- American Indian – Sappony
- American Indian – Occaneechi Band of the Saponi Nation
The above options will also be made available for parent(s) race and tribal affiliation for all births registered or amended in the NCDAVE Electronic Birth Registration System and issued by NCOVR beginning January 1, 2024.
According to the 2020 U.S. Census Bureau, more than 130,000 American Indians live in North Carolina, making it the seventh largest American Indian population in the United States.
"This change is long overdue and will help preserve the rich history of American Indian culture in North Carolina," said Rev. Ricky Burnett, Chairman of the NC Commission of Indian Affairs. "The Commission is committed to providing support for and advocating for North Carolina's American Indian population."
Governor Roy Cooper proclaimed November as American Indian Heritage Month, celebrating the history and heritage of the eight state recognized tribes in North Carolina. They are Coharie, Eastern Band of Cherokee, Haliwa-Saponi, Lumbee, Meherrin, Occaneechi Band of the Saponi Nation, Sappony and Waccamaw- Siouan.
Presentation of race and tribal affiliation on birth and death certificates will not impact the state's vital statistics reporting format to the Centers for Disease Control and Prevention National Center for Health Statistics.
More information about birth and death certificates in North Carolina can be found on the website https://vitalrecords.nc.gov.
More information about the NC Commission on Indian Affairs can be found on the North Carolina Department of Administration's website.
You can also learn more about national vital records reporting statistics on the CDC website.
NC Clinician and Physician Retention and Wellbeing Consortium is for YOU!
The North Carolina Medical Society (NCMS), through the North Carolina Clinician and Physician Retention and Wellbeing (NCCPRW) Consortium, aims to address unspoken physical, emotional, and mental areas of stress and burnout.
In 2024, one of the NCMS's priorities focuses on fostering health system environment changes that improve the daily lives of our members through the current and continued work of the NCCPRW Consortium.
The well-being of you, our healthcare clinicians, is not only a moral imperative, but also a fundamental necessity for the effective delivery of healthcare services.
As you all tirelessly work to save lives and provide comfort to those in need, it's essential that we prioritize your physical, mental, and emotional health. Visit the NCMS’s Wellness and Resilience page for additional resources to combat stress, burnout, clinic fatigue, and more.
In addition, there is a free Physician Support Line open Monday – Friday: 8AM – 12 AM ET at 1-888-409-0141, available to clinicians in need of an outlet, resources, or additional support.

Give the Gift of Leadership This Holiday Season! 🎄
Support the next generation of clinicians and aspiring leaders in health care!

Are you interested in making a meaningful contribution to the future of healthcare leadership? Consider becoming a sponsor for a student in the Future Clinician Leadership Course (FCLC) or a scholar in our esteemed Leadership College or Health Care Leadership & Management programs.
- Future Clinician Leadership Course (FCLC): By sponsoring a student in FCLC, you'll empower the next generation of clinicians to develop critical leadership skills early in their careers.
- Leadership College: Sponsorship for Leadership College scholars allows you to directly invest in individuals who are committed to shaping the future of healthcare leadership.
- Health Care Leadership & Management (HCLM): By sponsoring a scholar in HCLM, you'll be supporting healthcare professionals on their journey to becoming visionary leaders. Your contribution can help them drive innovation and improve healthcare delivery.
Why Sponsor? Your sponsorship goes beyond the financial aspect: It's a chance to nurture talent, inspire ambition, and foster the growth of leaders who will impact the healthcare industry positively.
Get Involved Today: To explore sponsorship opportunities and learn more about how you can make a difference in the lives of these emerging leaders, please reach out to Pam Highsmith, VP of Development at [email protected]. Your generosity will play a pivotal role in shaping the future of healthcare leadership.
Join us in our mission to empower the leaders of tomorrow and continue the legacy of excellence that defines the KIPL community. Together, we can make a profound difference in healthcare leadership.
Consider a sponsorship today. It's the gift that keeps on giving!
WCMS Hosts Historical Performance Where Past and Present Come Together
On Sunday November 19th, the Wake County Medical Society hosted a family event at Haywood Hall and Gardens in Raleigh, welcoming highly acclaimed veteran historical actor-interpreter Bill Barker, described as the nation's foremost interpreter of Thomas Jefferson.
Combining the tools of theater with rigorous historical scholarship, Barker explored Jefferson’s life and times, and how it relates to our world today.


7 More Days Until Giving Tuesday! Make Your 2024 Donation Plan Now!
After the back-to-back days of deals on Black Friday and Cyber Monday, join us in kicking off the holiday giving season on #GivingTuesday!
On the Global Day of Giving, we’re raising funds to improve the health and well-being of North Carolinians.
We want to be sure that ALL North Carolinians have an equal chance at healthy lives, and your involvement is essential.
Ways to gear up for #GivingTuesday:
- Donate. Lock in your gift now!
- Follow us on Facebook, Twitter and Instagram
- Share this message and our social media posts and encourage others to join the movement
We’ve got just one week left until the historic day of giving! Let’s do this!

Tips to Help Avoid Norovirus this Holiday Season
While Norovirus outbreaks can happen anytime, they usually occur from November to April. The virus spreads easily and quickly from infected people to others and through contaminated foods and surfaces. People of all ages can get infected and sick.
Taking a few precautions can help protect against the virus:
- Wash your hands often
- Rinse fruits and vegetables
- Cook shellfish thoroughly
- Stay home when sick and for two days after symptoms stop
- Avoid preparing food for others when sick and for two days after symptoms stop
The most common symptoms of Norovirus are diarrhea, vomiting, nausea, and stomach pain.
Learn more about Norovirus here.
Download a Norovirus Fact Sheet here.

Mark Your Calendar Now! Collaborative Care Model Learning Collaborative Planned for Early 2024
Collaborative Care Model (CoCM) Provider
Learning Collaborative
January 18, February 15, March 21, April 18, May 16, June 20, 2024
12:30 - 1:30 p.m. | Location: Livestream Webinar

The Collaborative Care Model (CoCM) is an integrated modality that provides patients with medical and behavioral health care in a primary care setting. The CoCM Learning Collaborative sessions will highlight collaborative care team integration and the role of the CoCM Behavioral Health Care Manager for practices new to the model and those established with implementing CoCM.
Objectives:
- Participants will be able to describe the principles of the Collaborative Care Model (CoCM).
- Participants will be able to identify key concepts and team member roles/responsibilities for effective implementation of CoCM.
- Participants will be able to explain the value and evidence for measurement-based, treatment to target CoCM care.
- Participants will be able to discuss the contributing factors to successful Collaborative Care implementation.
Target Audience:
These Learning Collaboratives are for primary care providers, behavioral health professionals, and anyone else who has implemented or is considering the Collaborative Care Model (CoCM) for integrating behavioral health in a primary care setting. Independent primary care practices, FQHC’s, and rural health clinics may find this collaborative especially helpful for meeting some of the behavioral health needs of their patients.
January 18, 2024 • 12:30 - 1:30 p.m.
Overview of CoCM Model/Role of PCP
February 15, 2024 • 12:30 - 1:30 p.m.
Role of the Psychiatric Consultant/Systematic Caseload Review
March 21, 2024 • 12:30 - 1:30 p.m.
Role of BH Care Manager/Registry Tracking
April 18, 2024 • 12:30 - 1:30 p.m.
CoCM Billing
May 16, 2024 • 12:30 - 1:30 p.m.
Communicating about CoCM Across the Care Team
June 20, 2024 • 12:30 - 1:30 p.m.
Caseload Management/Relapse Prevention Plan
Registration is required for each date via the link (participants will use this link for each session).
Download the PDF here.
For Additional information about the model please click this link.
Questions? Contact LaShawnna Andrews, MSM, Director, Continuing Professional Development IPE at (910) 678-7319 or [email protected]
In Memoriam: Former Wake County Medical Society Executive Director Paul B. Harrison
Paul B. Harrison, former Wake County Medical Society Executive Director, died Tuesday, November 14. He was 79.
Harrison served 21 years as the Executive Director of the Wake County Medical Society (WCMS). In the role, he worked to advance the WCMS mission of developing a medical care safety net for indigent residents of Wake County.
In 2021, Harrison's years of service to the Wake, and surrounding medical communities, were recognized with the John Huske Anderson Award, given annually to a layperson whose contributions have had a positive impact on the medical profession and public health.
Volunteerism became a big part of Paul’s life, with a focus on the least advantaged in our society. He served in the U.S. Peace Corps (Micronesia) and on the staff of the Peace Corps Agency in Washington, DC. In the Triangle, he served as a volunteer innkeeper at the Durham Ronald McDonald house, as a volunteer swim instructor for handicapped students in Chapel Hill, as a volunteer intake screener at the Wake County Open Door Clinic, and as a member of the boards of Urban Ministries of Wake County, The Triangle Community Foundation and Judea Reform Congregation in Durham.
Chip Baggett, CEO of the North Carolina Medical Society (NCMS) had this to say about Harrison: “It is rare to find a public servant who quietly goes about planting and nurturing the seeds of change. Paul’s contribution to the health and well-being of patients is enduring. I am grateful for his leadership.”
The North Carolina Medical Society extends its deepest sympathy to Harrison's family and friends.
Read Harrison's full obituary here.