

UNC Health "Socking it to" Parkinson's
Minges Wellness Center at UNC Health Lenoir is excited to announce the launch of Punching Through Parkinson’s, a non-contact unique boxing program designed specifically for individuals with Parkinson’s disease. This program aims to improve physical health, strength, balance, and overall quality of life through exercise tailored to the needs of Parkinson’s patients.
Parkinson’s disease can cause motor and non-motor symptoms that affect movement, coordination, and daily life. According to Parkinson Association of the Carolinas, nearly one million people are living with Parkinson’s throughout America and up to 10 million people worldwide. Men are one and a half times more likely to have Parkinson’s than women.
Research has shown that regular exercise, including boxing, can significantly reduce symptoms and improve overall well-being. Studies have shown that activities like boxing can help Parkinson’s patients improve motor function and coordination, enhance cognitive abilities and mental clarity, and boost overall energy and mood. The high-intensity nature of boxing training, combined with its focus on mental sharpness and physical movement, is ideal for combating the physical challenges of Parkinson's.
The program will be led by certified trainers within Minges Wellness Center who have experience in fitness and working with individuals with Parkinson’s disease. Each session will be modified to suit different fitness levels, ensuring every participant can engage safely and comfortably.
Punching Through Parkinson’s will require physician clearance and registration. The class is an at-cost program that starts at $40 per month. Classes will be around one hour long with 15 minutes of set-up and break-down at the beginning and end of class.
For more information or to register for Punching Through Parkinson’s, contact Minges Wellness Center at 252-522-7944. [source]

HHS, Cedars-Sinai Partner to Advance Civil Rights and Improve Maternal Health

Agreement Takes Important Steps in Addressing Racial Disparities in Maternal Health Outcomes by Ensuring That Black Women and Other Women of Color Have Access to Treatment During the Full Course of Their Care
The U.S. Department of Health and Human Services (HHS), Office for Civil Rights (OCR), and Cedars-Sinai Medical Center (Cedars-Sinai) entered into a Voluntary Resolution Agreement (Agreement) to improve maternal health outcomes for Black, Latina, and other maternal patients of color. In June 2022, OCR opened a compliance review of Cedars-Sinai based on concerns expressed by patients. This Agreement concludes OCR’s review into Cedars-Sinai’s compliance under Federal civil rights laws that prohibit discrimination on the basis of race, color or national origin, resolving allegations of racial bias in healthcare, treatment and access to health care services. OCR did not determine any violation of Federal law by Cedars-Sinai in its review. Title VI of the Civil Rights Act of 1964 (Title VI) and Section 1557 of the Affordable Care Act (Section 1557) are laws that prohibit discrimination on the basis of race, color, or national origin.
OCR initiated a compliance review in response to media reports and complaints alleging racial bias in maternal care at Cedars-Sinai. Prior to OCR’s compliance review, Cedars-Sinai had undertaken substantial efforts to understand and mitigate the effects of discrimination and bias in healthcare. For example, Cedars-Sinai instituted mandatory annual unconscious bias education for staff while creating internal quality improvement programs and collaborating closely with community partners to improve Black maternal health outcomes. Today’s Agreement demonstrates OCR’s and Cedars-Sinai’s shared goals of promoting health equity and eliminating bias and discrimination in healthcare.
To continue to full article, click here.

NC Medicaid: Claims Denial for Services with Identified Third-Party Insurance
NC Medicaid is implementing updates to NCTracks Third Party Liability (TPL) process for NC Medicaid Direct. These updates will impact claims submitted for certain services when a member has other third-party insurance coverage listed in their eligibility record.
What This Means for Providers
Claims for the following services will be denied if third-party insurance is detected in the member’s eligibility record:
- Hospice
- Private Duty Nursing
- Home Infusion Therapy
- Local Health Department (LHD)
- Therapy Services
- Institutional Ambulance
- Hearing Aid
- Independent Diagnostic Testing Facility/Portable X-ray
- Providers are required to submit these claims to the member’s primary insurer before billing Medicaid.
What Providers Need to do to Avoid Claim Denials
- Check Member Eligibility Before Billing: Always verify member eligibility and third-party insurance information in NCTracks prior to submitting claims.
- Submit Claims to Primary Insurance First: Ensure claims for the affected services are submitted to any identified third-party insurance before sending them to NC Medicaid.
- Maintain Documentation: Keep Explanation of Benefits (EOB) records from the primary insurers for audit and resubmission purposes.
Claims submitted prior to December 31, 2024, will not be affected. These updates align with NC Medicaid Direct federally mandated role as the payer of last resort.
Contact
Third Party Recovery; 919-527-7690

NCMS CEO Chip Baggett Featured in Podcast About Prior Authorization

Unpacking the Red Tape: How Prior Authorization Affects Patient Care
Smith Anderson has unveiled its new podcast, Pulse on Carolina Health, a platform dedicated to unpacking critical issues shaping the healthcare landscape in North Carolina.
In the inaugural episode, “Unpacking the Red Tape: How Prior Authorization Affects Patient Care,” health care attorney Robert Shaw sits down with Chip Baggett, CEO of the North Carolina Medical Society, to examine the complexities of prior authorization and its impact on patients and providers. Chip has been at the center of the major trends and policy discussions involving health care in North Carolina for almost 20 years and is an advocate for issues facing the medical community.
Prior authorization, originally intended to ensure clinical necessity for expensive treatments, has become a heated topic across the state and country. Chip explores its evolution from a cost-containment tool into a system that sometimes relies on algorithms, which raises questions about technology’s growing influence in medical decision-making. He discusses how this prior authorization shift has led to uncertainty about who is truly practicing medicine—the doctor, the insurer or the algorithm.
“We have to try to make sure that we’re not denying care to patients, that we’re not frustrating patients and leading them not to get care, and that we're not leading to more mental anguish when a patient is already in a tough spot and then told they can’t get the care the doctor says they need,” said Chip. “Those are some things that I think will drive innovation in this space.”
Podcast host Robert has extensive experience advising companies on health care and regulatory matters. He regularly handles complex restructuring, M&A work on the buyer side and seller side, Medicare and Medicaid audits, value-based care projects, tax planning and controversy, hospital joint ventures, employment agreements, corporate advice and regulatory compliance such as HIPAA, Anti-Kickback Statute, and Stark Law matters. He has been recognized in Chambers USA, Health Care (2023-2024) and The Best Lawyers in America®, Administrative/Regulatory Law (2023-2025).
American health care is undergoing an unprecedented transformation, and Smith Anderson’s team of experienced health care lawyers are committed to guiding medical professionals, hospitals, health care facilities and industry organizations through the attendant changes and evolving regulatory environment. We advise clients nationwide on health care policy, legislative advocacy, executive strategy, mergers and acquisitions, privacy and data security, litigation and the complex business requirements of organized medicine. We have been integrally involved in launching innovative health care delivery initiatives such as clinically integrated networks, joint ventures between health systems and practitioners, Community Care of North Carolina and Accountable Care Organizations (ACOs) nationwide.
Stay tuned for future installments, where industry leaders and experts will tackle the pressing challenges in today's complicated health care system.
Listen to the debut episode of Pulse on Carolina Health here.
Listen and follow this podcast:
Apple Podcasts; Spotify; or your favorite podcast app.

Registration Open for the 2025 UNC Eye Symposium
2025 UNC EYE SYMPOSIUM
The William & Ida Friday Center for Continuing Education
April 12, 2025
8:00 AM - 5:00 PM
The UNC Eye Symposium will provide the latest updates and insights in the diagnosis and treatment of eye disorders, including anterior segment, glaucoma, neuro-ophthalmology, ocular oncology, oculoplastic, retina, and pediatric ophthalmology.
Download (pdf) flyer for more information



NC Medicaid: January Tailored Care Management Provider Manual Updates

NC Medicaid has released updates to the January Tailored Care Management (TCM) Provider Manual. These updates aim to enhance clarity and provide flexibility for providers. Notable changes include:
- Clarification on Applicability of the Provider Manual to Tailored Plans / Local Management Entities/Managed Care Organizations (LME/MCOs)
- New Flexibility on Supervising Care Manager’s Role in Reviewing Care Plans/ISPs
- Revised Requirement on Timeframe to Complete the Care Management Comprehensive Assessment
- New Flexibility and Clarifications on the Process for Conducting the Care Management Comprehensive Assessment
- Clarification on Ability to Address Urgent Needs Prior to the Care Management Comprehensive Assessment
- Clarification on the Requirements for Reassessment
- Clarification on Care Manager’s Role in 1915(i) Care Coordination
The January Provider Manual update and summary of updates are available on the Tailored Care Management webpage under Provider Manual.
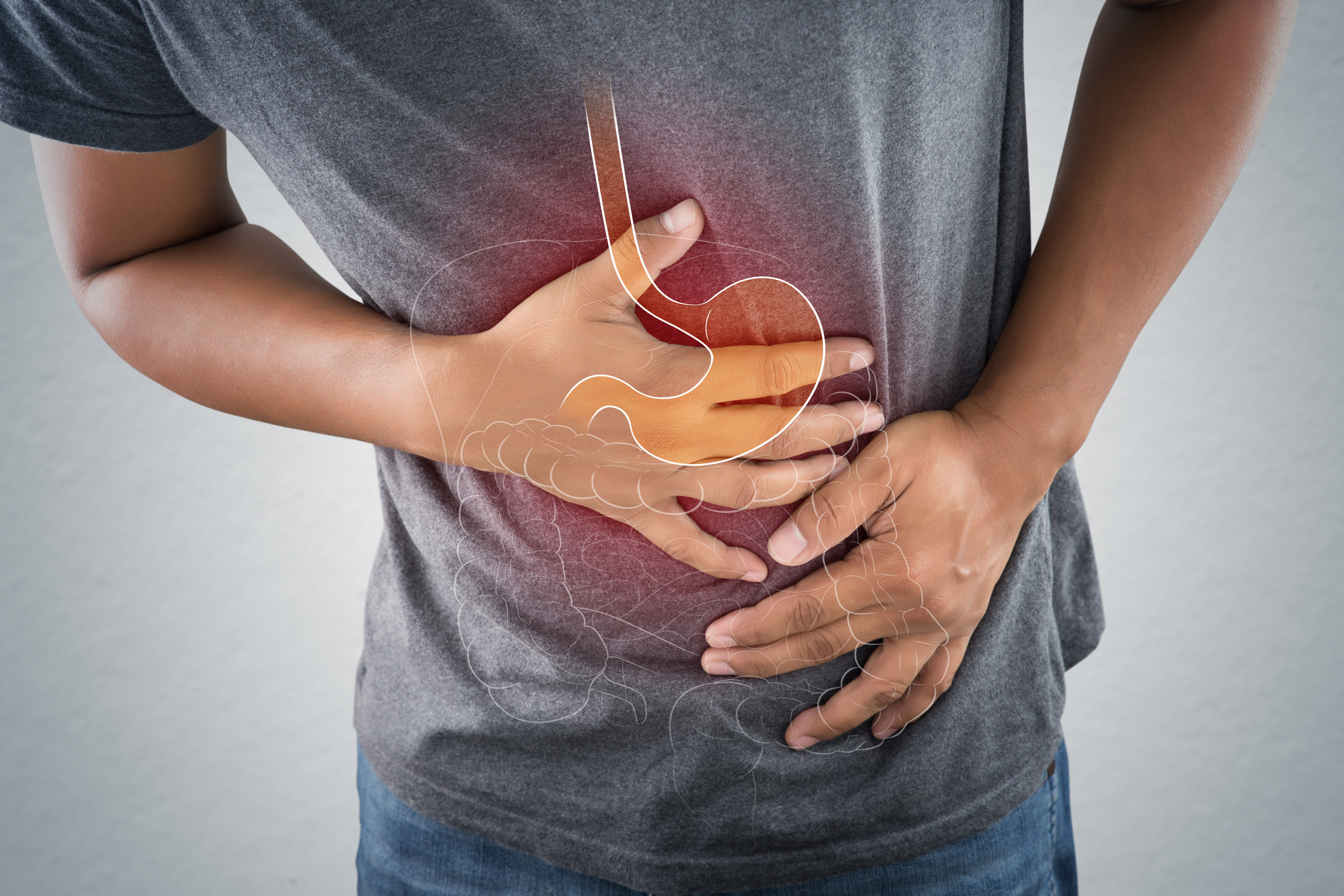
Eating More Fiber May Help Protect Against Dangerous Bacteria
Consuming more fiber, commonly found in whole grains, vegetables, and fruits, may help defend against harmful bacteria in the gut.
A recent study published in Nature Microbiology reveals individuals with high levels of the beneficial bacteria Faecalibacterium are more likely to have lower levels of harmful bacteria like E. coli. The research, which analyzed gut microbiome samples from over 12,000 people across 45 countries, highlights the potential health benefits of this particular microorganism.
The researchers also discovered that samples rich in Faecalibacterium contained elevated levels of beneficial compounds known as short-chain fatty acids, which are produced when fiber is broken down. Studies have shown that lower levels of this bacteria are associated with inflammatory bowel and gastrointestinal disorders.
Continue to full article here.

Tell the North Carolina General Assembly the Time is NOW to Pass Prior Authorization Reform!
Sign our petition to tell the North Carolina General Assembly, the time is NOW to pass Prior Authorization Reform.
Why reform Prior Authorization?
We've All Felt It. Every one of us, or someone we love, has had a hard time because of something called "prior authorization" in healthcare. Insurance companies use prior authorization to slow down or even stop people from getting the care they need. This is continuing to mess with people's lives.
Prior Authorization reform will allow for timely decisions to be made by the insurance companies, insurance companies must work with the patient's physician before denying coverage, and insurance companies must make prior authorization criteria clear and understandable.
By signing our petition, you are telling the North Carolina General Assembly the time is NOW to pass Prior Authorization Reform.


NCMS Member Pens Open Letter to People of Los Angeles

Hurricane Helene, which hit the East Coast last September, submerged Derek Moss' pediatric practice under 5 feet of water. He offers notes on grief and hope. | Flooding in the area around Hendersonville Pediatrics, in Hendersonville, North Carolina. courtesy of Jim Marshall.This article was first published in Zocalo Public Square
First, the Loss. Then, the Insurance
A Pediatrician Whose Office Flooded in Hurricane Helene Offers Los Angeles Notes on Disaster
Watching the images of fires burning in and around Los Angeles is very triggering. I’m sure it is the same for other Western North Carolinians. It has not been that long since Hurricane Helene caused catastrophic flooding that devastated our communities, and it is not over for us.
At first, you are energized to do what is needed to be done in the moment. But, then, you are left with emptiness, exhaustion, pain, trying to regain something resembling what has been lost.
These emotional twists and turns, highs and lows, have been a central part of my experience of natural disaster. How do you prepare someone for these head-spinning feelings, and for the aftermath, the trauma after the trauma of the weeks and months that follow? For the losses: Home? Business? Neighborhoods? Community? Routine? Safety? Life? For the total disruption.
In the beginning, you hear so many awful stories. People you know who have lost family members, friends. Those who have lost their homes. Places that are no longer there. Chimney Rock, the village I would drive my family through on our way to Lake Lure, gone. Highland Football Club’s soccer fields in Asheville, where our sons played, gone. Biltmore Village, where we have eaten, shopped, slept, gone.
And then there is your own story. My family was safe, and our house was fine, for the most part, but the office where I practice as a pediatrician—and which has served our community since 1952—was completely submerged under 5 feet of water. We lost everything on the first floor: walls, examination tables, files, flooring, cabinets, lab equipment, desks, nursing stations. Only the cement slab and the wall studs were left.
So what comes first is the loss. There are those who lose every possession or almost everything or about half of everything. Then there are those who don’t lose any things. They are still affected, but will sometimes, in conversation, almost seem to forget because they’re existing in a usual, comfortable state.
For many of us, after the loss, there is the insurance—or lack thereof. There are those here who didn’t have flood insurance. On the Carolina coast, when hurricanes destroy homes and buildings, it will be someone without wind insurance. In L.A., it may be that people don’t have the right type of fire insurance. If you do have the correct insurance, it takes months to get the money—that is, if your insurance company doesn’t go bankrupt.
My business, Hendersonville Pediatrics, has yet to receive one cent from an insurance company. We have four policies with two different providers—two of which are flood insurance policies.
People tell you the delay in insurance is the way it is. It’s the government, which runs our primary flood insurance program. It’s the paperwork. You’ve got to roll with it.
But, it’s money.
Money doesn’t drive everything or everyone. There are people who will appear out of nowhere to help. Heroes. The ones flying helicopters to pick people up off of mountains, defending dams, clearing roads, putting out fires, getting your power on, your cell phone service up, giving you your clean, safe water back. Our community has received such an influx of food, medicines, clothes, diapers, sanitary products—things you don’t think about until you don’t have them.
People from within your community appear to help, too—people you have never met before.
Pauline Carpenter at Free Clinics gave Hendersonville Pediatrics space for a doctor four days a week. Richard Hudspeth and the Blue Ridge Health administration allowed us to rent an office to house two doctors five days a week.
But these places are not home. At home, four doctors saw over 100 children, every weekday. People say they love children. But they don’t like hearing them screaming and crying. We are constantly worried: Are we quiet enough? Are they going to kick us out? It is something we cannot control. So we just keep working.
The disaster has not ended for us. It won’t, for years. It probably never will. Because things will never be as they were before. From now on, we know disaster can happen.
What do we do in the meantime? It is up to us in our communities to rebuild, to be the backbone, the strength. In our office, it’s been amazing how supervisors have stepped up to bring order to our practice. Staff changing their schedules. Everyone helping us rebuild our lab, our supplies, our vaccine inventory. That’s the beauty in this type of destruction. Neighbors helping neighbors. People being there for others. Being present. Being in this moment.

Capitol Chronicle: Telehealth Flexibilities for Medicare Patients Extended – Future Uncertain, Urgency Persists

Telehealth Flexibilities for Medicare Patients Extended – Future Uncertain, Urgency Persists
On December 20, 2024, Congress passed a short-term spending bill for the purpose of keeping the federal government operational through mid-March 2025. Our primary focus in working with our US House and US Senate members leading up to and during the bill’s debate was the inclusion of Medicare payment fix for physicians. From introduction to enactment, the bill was edited and the Medicare payment provision was ultimately eliminated. There was, however, an important measure that survived the bill edits – a temporary extension of Medicare telehealth coverage.
Section 3027 of the enacted federal funding legislation, H.R. 10545 / American Relief Act, entitled Extension of Certain Telehealth Flexibilities, keeps telehealth considerations under Medicare in place through March 31, 2025. Among those provisions are the following:
1. Audio-only services
2. Geographic and originating site requirements
3. Eligible providers
4. Mental health services
These and other provisions were implemented to maintain access to telehealth services for Medicare patients during the COVID-19 pandemic and public health emergency (PHE). In recognition of the positive impact of the flexibilities implemented, bipartisan health policy discussion on Capitol Hill has acknowledged the value of telehealth and has addressed continued support of the enacted flexibilities.
In March 2024 stand-alone bills that Congress considered last year – H.R. 7623 / S.3967 – Telehealth Modernization Act of 2024. This legislation proposed extending the telehealth coverages through 2026. These extensions follow what was included in the year-end funding package. North Carolina’s House and Senate members who signed on as co-sponsors of these bills included Congresswoman Deborah Ross, Congressman Wiley Nickel and Senator Thom Tillis. Comparable legislation is anticipated in 2025.
What hangs in the balance?
The Medicare telehealth flexibilities currently in place are scheduled to expire on March 31, 2025, if Congress enacts another extension or acts to make them permanent. The initial word from Capitol Hill is encouraging with regard to support of further extensions but there is uncertainty of the focus of cost-cutting targets under the new administration. A failure to extend the flexibilities will have an impact on physicians and other providers as well as patients. Notable flexibilities include:
Telehealth Delivery
Telehealth flexibilities currently allow for patient encounters via audio-only. Prior to the pandemic such engagement with required the use of two-way audio/video technology. An expiration of the Medicare telehealth flexibilities would eliminate the audio-only option.
Geographic/site of care requirements
As a result of the pandemic and the declaration of a public health emergency (PHE), flexibilities were extended to allow Medicare patients to receive care via telehealth at “any site in the United States at which the eligible telehealth individual is located at the time the service is furnished… including the home of an individual.” Eliminating this flexibility would result in an access to care issue for some patients, especially those in rural and underserved areas.
Providers eligible to provide telehealth services
Under the flexibilities extended as a result of the pandemic PHE, Medicare patients were allowed to access care via telehealth from an expanded list of providers, such physical therapists, occupational therapists, etc. If the flexibilities are not extended, the eligibility to provide telehealth services will revert to pre-pandemic rules and a more restricted list of approved providers, which would limit access to care.
Behavioral Health
Under the telehealth flexibilities Medicare patients receiving behavioral health care are eligible to obtain those services via telehealth with no in-person visit requirements. If the flexibilities expire, Medicare beneficiaries receiving mental health services via telehealth will be required to have at least one in-person visit every 12 months.
The outlook for 2025 is that an extension of coverage for Medicare telehealth services will be part of the discussion when Congress again engages in debate over funding of the federal government. Such action will be necessary early in the year since the current funding package expires in March. The reintroduction of standalone bills is anticipated as well.
Appointment Opening for the NC Medical Care Commission
![]()
The North Carolina Medical Society has the opportunity to nominate a member to be appointed by the Governor to the North Carolina Medical Care Commission.
The North Carolina Medical Care Commission of the Department of Health and Human Services consist of 17 members appointed by the Governor. Three of the members appointed by the Governor are nominated by the North Carolina Medical Society.
Learn more about the purpose of the NC Medical Care Commission here.
View the 2025 Schedule of quarterly meetings here.
NCMS Application to State Boards and Commissions here.
The Nominating and Leadership Development Committee (NLDC) will interview applicants virtually on the evening of Wednesday, February 26, 2025.
The deadline to submit NCMS Application for North Carolina Medical Care Commission: Wednesday, January 22, 2025.

🎉We're Celebrating New Members!🎉
Join us in welcoming these new members to the North Carolina Medical Society!
- Quentin E. Adams, MD
- Jacob C. Andrews, DO
- Jeffrey R. Ashton, MD
- Philip M. Barber, MD
- Darren A. Bates, PA-C
- Lisa Biswas, MD
- Carley D. Bloomfield, DO
- Brenn A. Bolding, PA-C
- Lindsey K. Cole, PA-C
- Marcus DiLallo, MD
- Joseph R. Dowd, III, DO
- Robert T. Duprey, MD
- Macie Edwards
- Erik A. Eklund, MD
- Caleb T. Epps, MD
- Sanaya Gandhi, PA-C
- Amol Garg
- Brooke Ann Gloria, MD
- David R. Guillen, MD
- Ashok K. Gupta, MD
- Kirsti L. Harris, PA-C
- Maria C. Hatara, MD
- Aubrey A. Hess, MD
- Jaclyn N. Hess, MD
- Olivia B. Hughes, MD
- Ivette E. Hurtado, PA-C
- Rayan N. Kaakati, MD
- Michael P. Kehoe, PA-C
- Farid M. Khan, MD
- Morgan E. Killian, MD
- Crysta I. Kyrazis, MD
- Frank A. Lacy, MD
- Andrew S. Laird, PA-C
- Shahmeer D. Lateef, MD
- Gabrielle G. Leonard, MD
- Johnathan S. Lowe, DO
- Abigail Maiorana-Boutilier, MD
- Dylan P. Matthews, MD
- Lauren E. Maxwell, PA-C
- Kaitlyn E. McDonough, PA-C
- Grant W. McKenzie, MD
- Ryan P. McLynn, MD
- Katherine Myers Dharmasri, MD
- Sarah B. Odom, PA-C
- Jason T. Owens, PA-C
- Nisarg A. Parikh, MD
- Evan C. Pohl, MD
- Yuri A. Pompeu, MD
- Danielle V. Price, DO
- Venkateswaran Ramakrishnan, MD
- Alexander B. Reddy, MD
- Jared J. Rejeski, MD
- Victor C. Showalter, MD
- Stephen B. Smith, MD
- Krista M. Stocke, PA-C
- Parker P. Suit, DO
- Rohit Sukumar, MD
- Carles R. Surles, Jr., MD, MPH
- Ekin Uzunoglu, MD
- Yun Wang, MD
- Morgan E. W. Warren, MD
- David G. Weatherford, MD
- David E. Weil, PA-C
- Matthew M. Yeager, MD
- James A. Yoder, MD
- Alexandra E. Zeitany, MD
We are thrilled to have you!
Not a member but would like to be? Joining is simple. Visit our membership center here.

The Fight Against Alzheimer’s Just Got Stronger: Moore Regional Hospital Introduces PET Amyvid Brain Scans
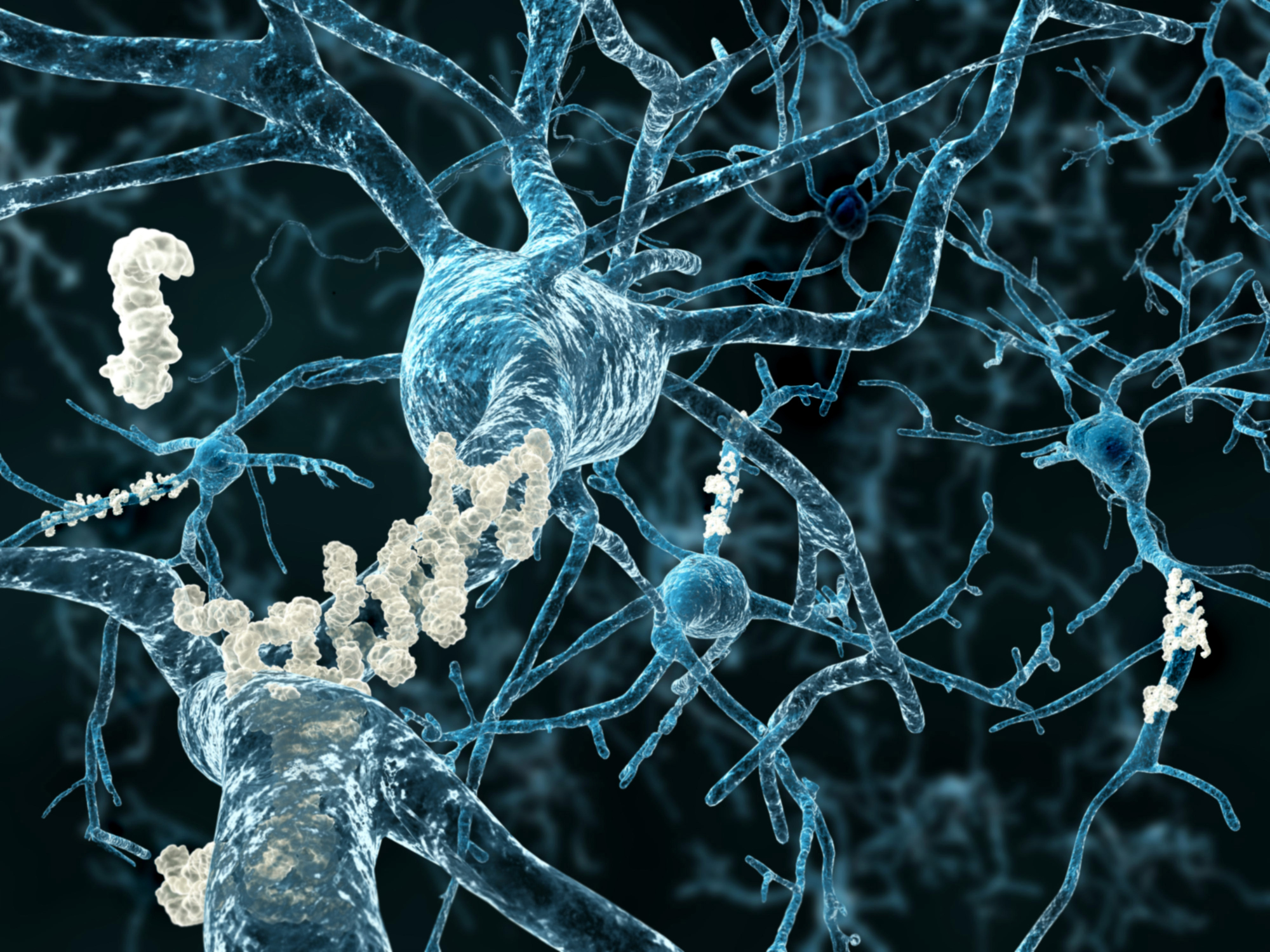
FirstHealth Moore Regional Hospital is proud to announce the availability of PET Amyvid brain scans, a cutting-edge diagnostic tool designed to detect beta-amyloid plaques, a hallmark of Alzheimer’s disease.
This advanced imaging technology offers new hope for earlier and more accurate diagnosis, empowering patients and their families to make informed decisions about care and treatment.
“The diagnosis of Alzheimer’s dementia requires a combination of history, exams, labs and imaging,” said Joshua Cho, M.D., interventional radiologist and nuclear medicine specialist with Pinehurst Radiology Associates. “While traditional imaging tools like MRI and CT focus primarily on anatomical markers, the PET Amyvid brain scan detects amyloid plaques, a biomarker strongly associated with Alzheimer’s. This capability sets it apart and gives us deeper insights into the disease.”
The PET Amyvid scan utilizes florbetapir, a synthetic compound that crosses the blood-brain barrier and binds to amyloid plaques.
“Florbetapir contains a radioactive isotope, F-18, which creates a signal detected by the PET scanner,” explained Dr. Cho. “This allows us to visualize the presence of plaques, although it doesn’t measure their quantity. It’s a significant step in understanding what’s happening in the brain.”
By identifying beta-amyloid plaques, the scan adds specificity to the diagnosis of Alzheimer’s disease and can help clinicians make earlier and more informed decisions about treatment. “This technology has the potential to improve outcomes,” said Dr. Cho. “If we can confirm the presence of amyloid plaques, we can start treatments earlier, which may help slow the progression of the disease.”
Moore Regional is one of only five hospitals in the state to offer PET Amyvid brain scans.
“The introduction of this advanced technology at Moore Regional Hospital underscores FirstHealth’s commitment to providing leading-edge diagnostics and care for patients,” said Kerri Fogle, MBA, MHA, CNMT, assistant director of nuclear medicine and PET imaging at FirstHealth Moore Regional Hospital.
Patients experiencing persistent or progressive unexplained mild cognitive impairment should consult with their primary care provider or neurologist to determine if this scan is appropriate. A referral from a neurologist is required. [source]

Disaster Energy Assistance Available to 25 Counties Impacted by Hurricane Helene
The North Carolina Department of Health and Human Services’ Low Income Household Energy Assistance Program (LIHEAP) began accepting applications from the general public for the Low Income Energy Assistance Program (LIEAP) on January 2, 2025. For the 25 counties that were heavily impacted by Hurricane Helene, additional Disaster Energy Assistance funding has been appropriated by the NC General Assembly to assist households with heating costs and repairs during the colder winter months.
Beginning January 15, 2025, applications for these additional Disaster Energy Assistance funds will be accepted for eligible households residing in one of the 25 identified disaster counties during and after Hurricane Helene. These counties are Alexander, Alleghany, Ashe, Avery, Buncombe, Burke, Caldwell, Catawba, Clay, Cleveland, Gaston, Haywood, Henderson, Jackson, Lincoln, Macon, Madison, McDowell, Mitchell, Polk, Rutherford, Transylvania, Watauga, Wilkes and Yancey counties.
Households can apply for both LIEAP and the Disaster Energy Assistance funding. Households with heating services or systems that require repairs, are currently inoperable, have been disconnected or are at risk of having their services disconnected can also apply for the Disaster Energy Assistance funds.
Eligible households will receive assistance based on household circumstances and need.
“Our friends and family in western North Carolina will feel the impacts from Hurricane Helene for years to come,” said Carla West, Division Director of Human Services for Child Support, Economic Services, Aging, and Operations. “We are only midway through winter, and these funds are critical to keep residents safe and warm as they continue to recover and rebuild.”
Disaster Energy Assistance is a temporary emergency program that helps eligible households and families afford energy heating services after a natural disaster or an emergency. The program provides assistance for eligible low-income households to provide, restore or continue heating sources. Disaster Energy Assistance is available until funds are exhausted.
Individuals in one of the identified 25 disaster declared counties can apply in-person or via telephone with their local county department of social services.
To be eligible for Disaster Energy Assistance, a household must have at least one U.S. citizen or eligible non-citizen and:
- Have income equal to or less than 60% of the state median income
- Have resided in one of the identified 25 disaster declared counties listed above during Hurricane Helene and are currently residing in one of those 25 counties
- Have been impacted and suffered a loss because of Hurricane Helene
Disaster Energy Assistance was created after NCDHHS was appropriated $9 million in state funds from the NC General Assembly to help assist these disaster areas with heating related costs and repairs as a result of Hurricane Helene.
ADDITONAL LINKS OF INTEREST

Register Now for Friday's North Carolina Infection Control Live Webinar
SPICE North Carolina Infection Control Course: Outpatient Healthcare Setting
January 24, 2025
8:40 AM - 3:45 PM
This approved infection control curriculum developed by SPICE prepares designated healthcare providers to ensure and systematically assess that their facility has the appropriate infection prevention policies and procedures in place to allow healthcare personnel to provide safe patient care consistent with the NC communicable disease rule .0206.
Objectives
- Discuss North Carolina state laws governing infection prevention in healthcare facilities.
- Describe control measures for Human Immunodeficiency Virus (HIV), Hepatitis B and Hepatitis C (10 A NCAC 41A .0202, .0203, and .0214.
- Review the importance of communicable disease reporting.
- Describe NC medical waste rules.
- Discuss bloodborne pathogen risks and other measures used for control of bloodborne pathogens.
- Review the Exposure Control Plan requirements.
- Discuss OSHA’s definition of regulated medical waste.
- Discuss best practices for safe injections and the consequences of unsafe injection practices.
- Discuss the One and Only Campaign to eliminate unsafe medical injections.
- Describe the best practices, principles and hand hygiene in asepsis.
- Explain the role of the environment in disease transmission.
- Discuss principals of disinfection and sterilization for medical devices used in outpatient facilities.
For more information and to register, click here.

Community Health Worker Supervisor Training Q&A
Community Health Worker Supervisor Training Q&A
January 28, 2025
11:30 a.m. - 12:30 p.m.
Curious about how to empower your role as a CHW Supervisor? Join this live Q&A session to explore what CHW Supervisor Training offers! The CHW supervisor training is provided by CHASM in partnership with SRAHEC and supported by the North Carolina Community Health Worker Association (NCCHWA). Training aligns with the competencies required for NCCHWA's Advanced Certification levels addressing factors across the Socioecological Model.
Download the brochure here.
Questions about this program?
Contact Justin Schwartz, MBA, BS, NREMT, CHW, Administrator, Continuing Professional Development / [email protected] / (910) 678-7286
NCMS Holds First Regional Meeting of 2025 in Fayetteville

Dozens of physicians and PAs meet to learn more about NCMS priorities and member benefits in Fayetteville
The North Carolina Medical Society held it's first Regional Meeting of 2025 at Luigi's Italian Chophouse in Fayetteville Thursday night.
A crowd of physicians, PAs, Residents , and Students gathered to hear the latest on how NCMS is fighting for them across the state. NCMS Board President, Dr. John Meier spoke to the crowd about how the NCMS is working on Prior Authorization reform, AI, physician burnout, and advocacy events planned for the year. He was followed by NCMS Board member Dr. Karen Smith who gave insight into her experience as an NCMS member and representative to the AMA. She also told the crowd about how the NCMS celebrates diversity and is welcoming to both physicans and PAs.
Other NCMS staff was on hand to answer questions about NCMS membership, NCMS leadership training opportunities, the Community Practitioner Program, and other NCMS perks of membership. Vice President of Advocacy John Thompson updated attendees on the upcoming focus on prior authorization reform and what NCMS is working on in the early days of the new General Assembly in Raleigh.
A robust question and answer session focused on prior authorization with questions that included what NCMS was doing, howe NCMS is working with the AMA on a host of issues, and about the NCMS efforts to bring physicians and PAs to rural and underserved areas of the state.

NCMS Recognizes NCMS Disaster Relief Fund Contributors

A heartfelt THANK YOU to these individuals and organizations for their contribution to the NCMS Disaster Relief Fund. Your generous donation is far more than just a financial contribution; it’s a lifeline for the many affected by Hurricane Helene, and vital in providing support to healthcare professionals and communities impacted by this disaster.
We invite you to spread the word about the NCMS Disaster Relief Fund and stay engaged with us as we work together to help restore our Western North Carolina neighbors.
We are grateful to have you in our community!
- Davis Moore Healthcare Practice Group
- Donald Irwin
- Patricia H. Petrozza, MD
- Cary C. Ward, MD
- Janice M. Westphal, MD
- American Medical Association Foundation
- Ana Ayala
- Katherine Beavers
- Sandeepkumar J. Gupta, MD
- Portia Marsh
- Physicians East, PA
- Bangladesh Medical Association of North Carolina
- Rebecca S. Carlin, MD
- Carolina Complete Health Inc.
- Anonymous
- James M. Provenzale, MD
- Moulton Family Fund
- Puraven Beauty and Wellness
- UBS Financial Services, Inc.
- Donald P. Wilcox
- American Medical Association Foundation
- Atlantic Internal Medicine
- Amar M. Amaresh, MD
- Edwin C. Bartlett, Sr., MD
- Deanna M. Boyette, MD
- Edwin K. Burkett, MD
- Cobb County (GA) Medical Society
- John A. Fagg, MD
- Barbara Hodde
- Martha G. Peck, MD
- Gary Price, MD
- Eugene E. Wright, Jr., MD
- Kathy F. Wright
- Curi
- Anonymous
- Christopher T. Grubb, MD
- Lyndon K. Jordan, III, MD, FACR
- Katie Lowry, MD, MPH
- Laura J. Luckadoo, MD
- Robeson Pediatrics
- Kirby Sheridan
- Catherine L. Sotir, MD
- Vinod C. Vallabh, MD
- Ian D. Archibald, MD
- Preecha Bhotiwihok, MD, MPH
- John W. Black, MD
- Anonymous
- Gay M. Bowman
- Georgi N. Brockway, MD
- Michael T. Brohawn
- Anonymous
- Carolina Complete Health Network
- Sharon M. Foster, MD, FAAP
- Donna C. Graves, MD
- M. Mark Hester, MD
- Suneya G. Hogarty, DO
- Marius J. Ilario, MD
- Linda W. Lawrence, MD
- Douglas S. McFarlane, MD
- Mark B. Moeller, MD
- Anonymous
- Raleigh Orthopaedic Clinic, PA
- Timothy J. Reeder, MD, MPH, FACEP
- Alan J. Rosenbaum, MD
- Anonymous
- Marshall Z. Schwartz, MD
- Douglas D. Sheets, MD, FACOG
- W. Alan Skipper, CAE
- Jennifer K. Stoddard, MD
- STUSQU, PLLC
- Lisa W. H. Thompson, MD
- Cheryl L. Walker-McGill, MD, MBA
- Craig E. Webb, MHS, PA-C
- Johnathan D. Williams, MD
- Anonymous
- Idil Aktan, MD
- R. D. Almkuist, II, MD
- American Board of Pediatrics Inc
- Caroline D. Ames, MD, FACS
- James H. Antoszyk, MD
- Joy Avery
- Timothy M. Beittel, MD
- Anonymous
- Anonymous
- Cedar Mount Behavioral Health, PA
- Center For Pain Management, PLLC
- Melissa M. Coale, MD
- Anonymous
- Kim D. Dansie, MD
- Jackie M. Davis-Jones
- Jessica F. Doerrler, PA
- Patricia Duncan
- Peter A. Eweje, MD
- Mark W. Featherston, MD
- Anonymous
- Joanne M. Fruth, MD
- Lisa M. Gangarosa, MD
- Highland Medical Associates
- Anonymous
- Joseph P. Hunstad, MD, FACS
- Kitsie Jones
- Christopher P. Jordan, MD
- Kerry Kendall
- Eugenie M. Komives, MD, FAAFP
- Ted R. Kunstling, MD, FCCP
- Andrew S. Lamb, MD
- Keith LaScalea, MD
- Anonymous
- Elizabeth G. Livingston, MD
- Anonymous
- Laura L. Martinez, MD
- Darlyne Menscer, MD
- Ashley Newton
- J. Thomas Newton, MD
- Carolyn O'Conor, MD
- Michael K. Patrick, MD
- Patricia Petrick, MD
- Emily Rayes-Prince, MD
- Anonymous
- Corianne D. Rogers, MD
- Nimesh B. Shah, MD
- Kristen M. Shipherd
- Maria J. Small, MD
- Anonymous
- Michol Stanzione, DO
- Steele Creek Dermatology
- Al Steren, MD and Diane Snyder Steren, MD
- Martha Strange, MD
- Thomas M. Swantkowski, MD, AGAF, FACG
- Marian L. Swinker, MD, MPH
- Christopher L. Tebbit, MD
- Monecia Thomas, PhD
- Dimitri G. Trembath, MD
- Michael J. Utecht, MD, FACEP
- Lynnea Villanova, MD
- Bonnie E. Wagner, PA-C
- Rebecca Y. Weinshilboum, DO
- Carl J. Westcott, MD
- Thomas R. White, MD
- Anonymous
- Women's HealthCare Consultant PC
- Nagarjuna Yerra, MD
- Michael Bartiss, MD / Family Eye Care of the Carolinas
- David Boone, MD
- Carolina Complete Health
- Karl Chiang, MD
- John Chretien, MD
- Anonymous
- Kelly Fedoriw, MD
- Carolyn Ferree, MD
- Alison Gardner, MD
- John Goldfield, MHS, PA-C
- Akilah Grimes, MD
- Sandra Jackson / Eastern Pediatrics
- Matthew Katz, MS / MCK Health Strategies
- Melissa Kenny
- Donna McGee, MD
- Larry Napolitano, Jr., MD
- Michael P. Reddy-Miller, MD
- Anonymous
- Andrew Pasternak, MD
- Antonio Ramirez, MD
- Beth Remhof
- Jennifer Root, MD
- Richard Savage, MD
- Anonymous
- Soma Sengupta, MD
- Nimesh Shah / Noble Hospitality Investment
- Amanda Trimpey, MD, MPH, FACOEM
- Yunxiang Zhu, MD
*Please note: List reflects donations received through Monday, January13, 2025.

Application Period Open for NCDHHS’ HBCU/MSI and Change Champion Internship Programs – Summer 2025 Cohort
The application period is now open for the 2025 NCDHHS’ Historically Black College/University and Minority Serving Institutions (HBCUs/MSIs) internship program's Summer Cohort. The application period closes on Thursday, February 20. The HBCUs/MSIs Internship program, in coordination with the Division of Public Health, is a component of the department’s workforce development initiative that encourages college students to seek careers in public health and human services in government agencies.
The program is recruiting students from HBCUs and MSIs in North Carolina to allow more equitable opportunities for internship access within NCDHHS, which supports building a strong and inclusive workforce, one of NCDHHS' strategic priorities. The program allows interns to learn more about what public health professionals, public administrators, social workers, and policymakers do at NCDHHS. In-person, hybrid and remote positions with experiential and project-based options are available.
Multiple internships are available for the HBCUs/MSIs Internship program. Sophomores, juniors, seniors, graduate and professional students and/or public health and human services majors are encouraged to apply. Undergraduate interns will be paid $20 per hour, and graduate or professional students will be paid $25 per hour.
The positions have broad requirements, such as the ability to engage and interact with internal and external partners; compile, assimilate and organize printed and electronic information; knowledge of data collection, organization to create reports, charts and other materials; the ability to present ideas clearly and effectively in written and verbal formats, as well as other requirements. Interns will work 40 hours per week, Monday through Friday between 8 a.m. to 5 p.m. Remote and hybrid options are available.
To apply for the HBCU/MSI Internship program, complete the Summer 2025 - Internship Interest Form. You must also email the NC State Government Application to [email protected] by February 20.
If you have questions about the NCDHHS HBCUs/MSIs Internship program, contact HBCUs/MSIs Program Manager Donyea Daniels at 984-303-6834 or Michael Leach, Senior Advisor, at 919-527-7536. You may also email questions/concerns to [email protected].

DEA & HHS Publish Final Rule on Telemedicine Prescribing for OUD

The Drug Enforcement Administration and the US Department of Health and Human Services will be publishing a Final Rule in the Federal Register on January 17, 2025, for prescribing of buprenorphine via telemedicine.
According to the new rule, providers will be permitted to prescribe a six-month initial supply of Schedule III-V medications to treat opioid use disorder via audio-only telemedicine interaction without a prior in-person evaluation. The rule also outlines allowances for follow-up medication prescriptions via telemedicine
The rule will become effective 30 days after publication. Below is a summary, which appears in the rule text.
https://public-inspection.federalregister.gov/2025-01049.pdf
The Drug Enforcement Administration and the Department of Health and Human Services are amending their regulations to expand the circumstances under which practitioners registered by the Drug Enforcement Administration are authorized to prescribe schedule III-V controlled substances approved by the Food and Drug Administration for the treatment of opioid use disorder via a telemedicine encounter, including an audio-only telemedicine encounter. Under these new regulations, after a practitioner reviews the patient’s prescription drug monitoring program data for the state in which the patient is located during the telemedicine encounter, the practitioner may prescribe an initial six-month supply of such medications (split amongst several prescriptions totaling six calendar months) through audio-only means. Additional prescriptions can be issued under other forms of telemedicine as authorized under the Controlled Substances Act, or after an in-person medical evaluation is conducted. This regulation also requires the pharmacist to verify the identity of the patient prior to filling a prescription. The Ryan Haight Online Pharmacy Consumer Protection Act of 2008 generally This document is scheduled to be published in the Federal Register on 01/17/2025 and available online at https://federalregister.gov/d/2025-01049, and on https://govinfo.gov requires an in-person medical evaluation prior to issuance of a controlled substance prescription. However, this regulation falls under one of the exceptions found within the Ryan Haight Act. Additionally, this regulation does not affect practitioner-patient relationships in cases where an in-person medical evaluation has previously occurred. The purpose of this regulation is to prevent lapses of care by continuing some of the telemedicine flexibilities that currently exist for those patients seeking treatment for opioid use disorder.

US Faces 'Quad-Emic' as Four Viruses Surge Simultaneously
Four viruses are surging across the U.S., prompting health experts to sound alarms about a potential 'quad-emic.'
As cases of influenza, respiratory syncytial virus (RSV), COVID-19, and a surge in norovirus continue to climb, the increase in illnesses is concerning, as these viruses can require hospitalization — or even be fatal — if not prepared for or treated properly. Hospitals are bracing for a strain on resources, with fears growing over the impact of multiple viral outbreaks occurring simultaneously.
There are vaccines for the respiratory viruses COVID-19, influenza, and RSV, but currently no vaccine for norovirus, which is commonly called the stomach flu but is not caused by influenza. Here are ways to keep yourself, your family, and your patients safe.
Children and Family Specialty Plan to Launch in 2025
The first-of-its-kind Children and Families Specialty Plan will go live December 1, 2025. This is a single, statewide NC Medicaid Managed Care plan that will wrap Medicaid-enrolled children, youth and their families in the child welfare system with seamless, integrated and coordinated health care.
NCDHHS and Blue Cross NC’s highest priority is to deliver a plan that meets the needs of the children and families of North Carolina and are committed to building the systems and processes needed to ensure the Plan works for families and the counties that serve them. Since the contract was awarded in August 2024, the two organizations have been working together and carefully planning to ensure the launch of the new plan goes smoothly and is ready to serve beneficiaries on day one.
For more on this new plan, click here.

NCTracks: Use of State License Boards Instead of Transcript to Verify Education and Training
Currently, when completing an Enrollment Application or Re-verification Application, NCTracks requests that some providers have their school send transcripts as proof of the highest level of education entered on the application. Effective November. 8, 2021, state licensing agencies that primary source verify education and training and display the information on their websites will be used as verification of education and training in lieu of a transcript.
See the table here (pdf download) for a list of state license agencies that can be used as verification of education and training. If "YES" is indicated in the PSV Education column, NCTracks will verify education and training using that source instead of sending a transcript request to the provider. If "NO" is indicated in the PSV Education column, transcripts will still be required.
For applications submitted prior to January 8, 2025, providers must still have their school send a transcript if one has been requested.

Join us in Raleigh on March 1 for the NCMS Advocacy Summit! Secure Your Spot Today!
Whether you're a healthcare professional, community leader, or passionate individual, the NCMS Advocacy Summit provides a platform to discuss, learn, and collaborate on shaping the future of healthcare.
We are thrilled to invite you to the NCMS Advocacy Summit, a groundbreaking event dedicated to exploring and advancing crucial topics in healthcare. Join us on Saturday, March 1, 2025, from 9 am to 5 pm at the StateView Hotel, located at 2451 Alumni Drive, Raleigh, NC 27606.
Event Highlights:
- Engaging Sessions: Delve into discussions on Access to Care Solutions, Corporate Practice of Medicine, AI in Healthcare, and much more!
- Diverse Perspectives: Gain insights from esteemed speakers representing various states and local community leaders, providing a comprehensive view of healthcare advocacy.
- Networking Opportunities: Connect with professionals who share your passion for healthcare advocacy. The last session of the day will be a townhall allowing leaders from specialty and county societies to speak.
Registration is Open, but Space is Limited! Don't miss this opportunity to be part of a transformative event. Secure your spot today by registering today!
We look forward to your participation in this impactful event.

Breaking: FDA Bans Red Dye No. 3 From Food, Drinks, and Ingested Drugs in US

Red dye No. 3 is found in some candy, food, drugs, and ingested beverages in US
(CNN, Kristen Rogers) -- The US Food and Drug Administration has banned the use of red dye No. 3 in food, beverages and ingested drugs, more than 30 years after scientists discovered links to cancer in animals, the agency announced Wednesday.
A synthetic color additive made from petroleum and chemically known as erythrosine, red dye No. 3 is used to give foods and beverages a bright cherry-red color.
The move acts on a November 2022 petition submitted by multiple advocacy organizations and individuals, including the Center for Science in the Public Interest and the Environmental Working Group, which cited links to cancer. The decision by the federal agency also follows in the footsteps of California, whose government banned the additive in October 2023.
Manufacturers using red No. 3 in food and ingested drugs have until January 15, 2027, and January 18, 2028, respectively, to reformulate their products, according to the FDA. Foods imported to the United States also must comply with the requirements.
“Today’s action by FDA is long overdue, is a small step in the right direction, and hopefully signals a renewed effort by FDA to do its job despite the many barriers the food industry places in its way,” said Dr. Jerold Mande, adjunct professor of nutrition at the Harvard University T.H. Chan School of Public Health, via email.
The decision marks a “monumental victory” for consumer health and safety,” said Ken Cook, cofounder and president of the Environmental Working Group, in a news release. “We wouldn’t be celebrating this historic decision today without the relentless leadership of public health champions like Michael Jacobson and others who took up this fight decades ago on behalf of consumers.”
Red dye No. 3 is found in at least dozens of candy, food and beverage products, but some of the most popular brands either never used, or have already stopped using, the additive. Fewer than 10% of products made by the candy company Ferrara, which produces Brach’s candies, for example, contain the additive, as the company began phasing out the use of it in early 2023, a Ferrara spokesperson said via email.
Just Born, the company behind PEEPS, stopped using red dye No. 3 in its production after Easter of 2024, according to a spokesperson.
Some companies instead utilize red dye No. 40, which has been considered a healthier alternative as it hasn’t been as extensively associated with cancer in animals.
However, California also banned red No. 40 from foods and drinks sold in public schools in September due to concerns over links to behavioral and attention difficulties among children. One study found a potential link to accelerated immune-system tumor growth in mice, and other sources say the dye contains benzene, a known carcinogen.
‘The regulatory paradox’ of dye red No. 3
Red dye No. 3 has been permissible for use in food despite the Delaney Clause of the FDA’s Federal Food, Drug, and Cosmetic Act. The clause, in part, “prohibits the FDA from approving a color additive that is ingested if it causes cancer in animals or humans when ingested,” according to the agency.
The FDA already banned the use of red dye No. 3 in cosmetics and topical drugs in 1990 under the Delaney Clause after research found the additive to be carcinogenic at high doses for rats in lab tests. The mechanism for the dye causing cancer in rats doesn’t occur in humans, so those studies didn’t raise safety concerns, and therefore the FDA didn’t revoke the authorization for red dye No. 3 in food, according to the agency.
The FDA has reevaluated the ingredient’s safety multiple times since its initial approval — based on trials conducted in animals, not humans — in 1969, according to the agency.
There don’t appear to be any studies establishing links between red dye No. 3 and cancer in humans, and “relevant exposure levels to FD&C Red No. 3 for humans are typically much lower than those that cause the effects shown in male rats,” the FDA said in its constituent update posted Wednesday. “Claims that the use of FD&C Red No. 3 in food and in ingested drugs puts people at risk are not supported by the available scientific information.”
But “it doesn’t matter, because the FDA mandate under the Delaney Clause says that if it shows cancer in animals or humans, they’re supposed to keep it from the food supply,” said Dr. Jennifer Pomeranz, associate professor of public health policy and management at New York University’s School of Global Public Health.
The FDA’s decision to revoke the authorization for the use of red dye No. 3 is a matter of law, the agency said.
A few other studies have cast further doubt on the safety of red No. 3, including a 2012 report that found a link between the additive and cancer in animals. That same year, researchers concluded artificial food colorings “are not a main cause of (attention deficit hyperactivity disorder), but they may contribute significantly to some cases, and in some cases may additively push a youngster over the diagnostic threshold.”
Then in 2021, the California Office of Environmental Health Hazard Assessment study found red dye No. 3 can make children vulnerable to behavioral issues, such as decreased attention. The report also concluded that federal levels for safe intake of food dyes at that time may not protect children’s brain health. The study noted that the current legal levels, set decades ago by the FDA, didn’t consider new research, according to the Environmental Working Group.
The FDA’s decision “ends the regulatory paradox of Red 3,” said Dr. Thomas Galligan, principal scientist for food additives and supplements at the Center for Science in the Public Interest in Washington, DC. But the agency “has a long way to go to reform the broken system that allowed Red 3 to remain in foods decades after it was shown to cause cancer when eaten by animals.”
The ban also moves the food landscape slightly closer to that of the European Union, which banned the dye in 1994, with the exception of some maraschino cherry products, Pomeranz said. “Europe takes the precautionary principle when it comes to these things.”
“There is not a rational reason within FDA’s mission that they did not ban red dye #3 from food in the 1990s,” and why the agency takes “so long to ban ingredients with known health harms” is unclear, Pomeranz said via email.
At least 10 other states — besides California — have introduced legislation seeking to ban red No. 3 from foods, according to the Center for Science in the Public Interest.
“Americans are sick because of our food,” Mande said. Though the United States is one of the wealthiest nations, in terms of overall life expectancy, the nation ranks as 49th out of 204 countries.
“This is because food companies have lost sight of their primary mission, providing food we will thrive on, and focusing entirely on their profits instead,” Mande added. “Unfortunately, the U.S. government doesn’t fund the research needed to determine the exact health risks posed by Red Dye #3. Industry works with Congress to block funding for the needed research.”
The National Confectioners Association said in a statement that food safety is the number one priority for US confectionery companies.
“Our consumers and everyone in the food industry want and expect a strong FDA, and a consistent, science-based national regulatory framework,” the association said via email. “For years, our industry has been calling for more transparency, more funding, and more staff resources for the FDA to continue fulfilling its mission, and it’s time to put politics aside and work together to fund the FDA at levels that will allow it to continue its work.”
Food and beverage companies will continue to follow the latest science and comply with all food safety regulations to ensure safe and available choices for consumers, Sarah Gallo, senior vice president of product policy and federal affairs at the Consumer Brands Association, said in a statement via email.
Avoiding dyes in your diet
The FDA has already required manufacturers to list red dye No. 3 as an ingredient on food labels — so if you’re concerned about avoiding products containing the dye until the ban is implemented, check ingredient lists before buying. Red dye No. 3 is also listed as “red 3” and “FD&C Red #3.”
Artificial food colorings are mostly found in ultraprocessed foods and beverages you couldn’t make at home, Pomeranz said, so avoiding those products is another way you can eliminate red dye No. 3 from your diet. The Center for Science in the Public Interest recommends parents avoid all numbered dyes, such as yellow No. 5 and red No. 40, as well.
You can find out how much ultraprocessed food you may be eating by taking this quiz.
For medications that aren’t topical, look for dyes in the “inactive ingredients” section of the drug labeling or package insert, or search for dye-free versions of some drugs, Consumer Reports suggests. But always talk with your doctor before switching medications.
New Survey: Radiation Oncology Burden of Prior Auth in 'Dark Place' - Sign Petition for NC Reform
Survey shows radiation oncology in ‘dark place’ as prior authorization burden worsens
(Healio News, Josh Friedman) -- An American Society of Radiation Oncology survey has shined a spotlight on the impact prior authorization has on providers and patients.
Nearly one-third of the more than 750 radiation oncologists who participated in the survey indicated prior authorization delays led to ED visits, hospitalization or permanent disability for their patients.
In addition, 7% of respondents reported prior authorization contributed to the death of at least one of their patients.
The findings — including the “inordinate number of deaths” — highlight the growing burden prior authorization is causing, according to Fumiko Chino, MD, assistant professor in department of radiation oncology at The University of Texas MD Anderson Cancer Center and Healio Women in Oncology Peer Perspective Board member.
“This is our 2024 temperature check to see where we are and, unfortunately, it shows that we’re in a very dark place,” Chino told Healio.
“We know the patients we have had that prior authorization killed,” she added. “We have them in our hearts.”
‘Who’s watching the watchmen?’
Prior authorization can provide benefit, Chino said.
Some clinicians may use outdated information to dictate treatment, or they may not stay up to date on technological or medical advancements.
The current fee-for-service payment model means that providers get “paid per treatment,” and that may incentivize certain longer regimens, Chino said.
“If the structure of your facility is built on doing 30 treatments for breast cancer, it’s harder to figure out how to keep the lights on in 15 treatments,” Chino said.
Prior authorization’s value comes from “utilization management,” Chino said. It is intended to “[make] sure the treatments that we’re providing for our patients are truly evidence based, and that they will help and not harm them.”
She cited American Board of Internal Medicine’s Choosing Wisely campaign as an example of appropriate resource stewardship. For radiation oncology, it includes consideration of shorter treatment fractionalization or not using radiation at all.
However, she said prior authorization has seemingly been used to mitigate increasing costs of care without consideration of its effects on patients living longer, better lives.
“[Prior authorization] is the guardrails on our physician prescribing, but what we found is that there’s no guardrails on the guardrails,” Chino said. “Who’s watching the watchmen?”
Survey background
ASTRO received online survey responses from 754 radiation oncologists between September and October 2024.
Respondents represented both private practices (51%) and academic institutions (47%).
About half of radiation oncologists who responded to the survey served in urban communities (49%), with more than one-third practicing in suburban (39%) areas and 13% practicing in rural areas.
According to the survey, 85% of radiation oncologists said the prior authorization burden has “increased greatly” (60%) or “increased somewhat” (25%) in the past 3 years.
Additionally, 94% said it worsens staff burnout “significantly” (57%) or “somewhat” (37%).
These issues forced 80% of respondents to reallocate staff time to deal with prior authorization requests, and 64% had to hire more employees.
Radiation oncologists reported several issues involving care, as well:
- 92% said prior authorization delayed treatment;
- 68% said those delays lasted at least 5 days, up from 52% in 2020;
- 82% reported it caused them to use a less-optimal treatment;
- 62% said they have to use less-optimal treatment in more than 10% of cases, up from 32% in 2019;
- 58% said it forced them to not follow recommended guidelines;
- 33% reported patients stopped radiation due to prior authorization;
- 30% said prior authorization led to adverse events, including ED visits, hospitalization and disability; and
- 23% reported they had difficulties getting approval for anti-nausea medications.
“Virtually every person I see will have some sort of prior authorization that is required,” Chino said. “Whether that is a barrier and causes a delay is quite variable but, ever since the COVID-19 pandemic, the prior authorization burden we’ve been seeing in our patient clinics, institutions and societies have only gotten worse.”
‘Meaningful’ improvements
On the positive side, 77% of respondents said more than half of their prior authorization requests went through on the first attempt. That number increased from 69% in 2019.
Additionally, 76% reported more than half of their requests that initially got denied received approval on appeal, up from 62% in 2019.
On average, respondents said 71% of prior authorization requests received initial approval, and 73% that initially got denied received approval on appeal.
“I think there’s this idea that if you just say no, some amount of people will just give up,” Chino said. “They don’t have the resources to do the appeals, or they don’t have the knowhow to understand that you have to work the system to get this approved.
“Making it to the appeal is really important, but that takes resources,” Chino added. “It takes time, and I can’t see a patient or make an elegant radiation plan in that time where I’m arguing with insurance companies. At some point, it can’t just be me and my staff fighting.”
Chino identified multiple ways the process could improve.
Although an expedited appeal occurs within 72 hours — a significant improvement from a few years ago — another reduction could be “really meaningful,” Chino said.
“I’ve had patients who’ve literally had a tumor growing out of their chest,” she said. “Waiting 3 days for an appeal means there’s more cancer to treat, even just in the time between when I made the plan for them initially, and when I actually get to start their treatment. Sometimes it means the plan has to change because the tumor has gotten that much bigger in that time period. Every day matters.”
Insurance companies could also green light regimens that are always approved on appeal, Chino said. This is the concept of the Gold Card system, which has made some headway at the state level.
“Can we maybe not spin our wheels and delay patients, and just facilitate those plans that are going to be approved?” Chino said. “Why are you making the patient wait?”
Payment reform could benefit care, as well.
“ASTRO has a proposed payment model that we put forward that would essentially be bundled payments. It’s a case rate based system,” Chino said. “I want to treat someone with breast cancer in 15 treatments. This person wants to treat them in 30 treatments. Whichever is best for the patient you can do, but you’re going to get paid the same thing.”
Institutions can take their own steps to improving the prior authorization process, as MD Anderson has done, Chino said.
“It has to do with taking a deep dive in the most common insurance providers,” she said. “Looking at what are the things they point to as the reason why they’re denying X, Y or Z plan, and then making sure that we’re showing clearly why this needs to be approved, based on your own criteria. It is a lot of work. It’s a lot of investment, but I do think it benefits patients and the institution with facilitated care.”
In the end, she said growth can only occur if all parties work together to solve the problem.
“We can’t keep pointing fingers,” Chino said. “The doctors point to the insurance and the insurance points to the [pharmacy benefit managers], and then everyone points at the government. It would be nice if we could all just work together to improve care. I feel like it really would benefit people.”
Tell the North Carolina General Assembly, the time is NOW to pass Prior Authorization Reform. Sign the petition!
Reference:
- ASTRO. How prior authorization harms cancer care: Results of a nationwide study, Dec. 24. Published Dec. 4, 2024. Accessed Jan. 9, 2025.

Grant Opportunity for State Designated Rural Health Centers

These grant funds, supported through the North Carolina General Assembly, allow ORH to partner with local communities to provide funding to improve their ability to serve underserved populations who would otherwise be unable to access needed primary care services due to geographic, economic, or other barriers. State Designated Rural Health Centers have become an integral part of the health care safety net for North Carolina’s rural and underserved residents.
Requests are contingent upon availability of program funding. ORH anticipates that approximately 15 applicants will receive funding. Successful applicants will be required to attend a grant award workshop.
The applicant organization must first assess if it can meet certain criteria. The purpose of the SDRHC program is to increase access to primary care for rural, uninsured, and underinsured residents.
More information, including how to apply, is available here.
Register Now! Essentials of Pain Management CME Event
![]()
On March 1, 2025, NCS-ACOFP and the Pain Societies of the Carolinas will host a one-day CME event in Raleigh, NC at the Campbell University Norman Adrian Wiggins School of Law.
The conference is titled: Essentials of Pain Management. Conference content will meet the NC licensure and DEA MATE Act requirements related to prescribing opioids and related topics. Learn the latest techniques, treatments, and options in acute and chronic pain management. Review the conference agenda here. The following CME credit types will be awarded: up to 8 AOA Category 1-A credits AOA and 8 AMA PRA Category 1 Credits™ .
Register by January 31, 2025, to take advantage of the Early Bird Registration Rates. Here is the link to register. Note: registration is done via the site of the Pain Society of the Carolinas.
Need Additional Information about the Conference?
Visit the NCS-ACOFP website or contact Nancy Guy, Director at [email protected] or by phone at 910-658-6501.
Take Action on Prior Authorization NOW! Sign Our Petition Today!
Sign our petition to tell the North Carolina General Assembly, the time is NOW to pass Prior Authorization Reform.
Why reform Prior Authorization?
We've All Felt It. Every one of us, or someone we love, has had a hard time because of something called "prior authorization" in healthcare. Insurance companies use prior authorization to slow down or even stop people from getting the care they need. This is continuing to mess with people's lives.
Prior Authorization reform will allow for timely decisions to made by the insurance companies, insurance companies must work with the patient's physician before denying coverage, and insurance companies must make prior authorization criteria clear and understandable.
By signing our petition, you are telling the North Carolina General Assembly the time is NOW to pass Prior Authorization Reform.

The Future of Psychedelic Use in Healthcare
Last year was tumultuous for the psychedelic medicine industry. Marked by the FDA’s rejection of Lykos Therapeutics’s MDMA-based depression treatment, experts project 2025 will be much more inconsequential, as companies are set to focus on recalibrating to avoid a similar fate.
Lykos’s MDMA therapy was widely expected to be the first FDA-approved psychedelic medicine. But the FDA rejected the company’s application in August, citing concerns about the data submitted. Lykos later agreed to complete a second Phase 3 clinical trial, though it has not announced when it would be able to resubmit its application for approval.
The agency’s decision showed that the psychedelic medicine industry still has a lot to prove to gain mainstream acceptance. But 2025 is off to a positive start, according to Lynn Marie Morski, president of the Psychedelic Medicine Association, pointing to the American Journal of Psychiatry dedicating its January edition entirely to psychedelic medicine.
“It was great to see such a long-standing organization from the mainstream medical side giving legitimacy to psychedelic medicine in that way,” Morski told Healthcare Brew. “It seems like this year is starting with an acknowledgement by some of the mainstream medical associations that…psychedelic medicine is a legitimate form of therapy.”
One of the main theories behind using psychedelic medicine to treat mental health conditions is that the drugs get to the root cause of conditions like anxiety or depression rather than just treating the symptoms, Morski told Healthcare Brew in May 2024. Providers could refer patients to various types of psychedelic therapy if they don’t respond well to traditional treatments, like SSRIs for depression.
For the full article, click here.

New Scholars Program Supports Local Health Sciences Students
image credit: Haywood Regional Medical Center
Haywood Regional Medical Center (HRMC) and Haywood Community College (HCC) are excited to announce the launch of a new Scholars Program, designed to provide a final dollars scholarship for health sciences students in exchange for a commitment to employment at HRMC upon graduation. The agreement will support students enrolled in the Registered Nurse, Nurse Aide I, Medical Assistant, Phlebotomy, and Paramedic programs at HCC, offering a pathway to stable, fulfilling careers in the healthcare field within Haywood County.
Through this partnership, program participants will receive financial assistance to complete their education, allowing them to stay within the local community to pursue career opportunities that contribute directly to the health and well-being of Haywood County residents.
Continue to full article here.

Reminder: Don't Miss the BCBS Antitrust Settlement Webinar on Thursday, January 16.
Physicians, medical groups, and health care facilities may be eligible to submit a claim as part of the settlement reached with the Blue Cross Blue Shield system.
In 2024, a settlement was reached in a long-running class action lawsuit against Blue Cross Blue Shield (BCBS) brought by physicians, hospitals, large health systems and provider organizations. The lawsuit alleged a range of antitrust violations by BCBS, including price fixing and allocating markets using exclusive service areas. In addition to $2.8 billion in damages, the Settlement Agreement requires BCBS to make hundreds of millions of dollars in investments to improve claims processing, including the processing of BlueCard claims.
Physicians, medical groups and health care facilities may be eligible to submit a claim as part of the settlement reached with the BCBS system if they provided health care services, equipment or supplies to Blue Plan patients between July 24, 2008, and October 4, 2024.
Whatley Kallas, LLP will host a webinar for medical providers on how to submit claims.
Medical Professionals/Groups: Thursday, January 16, from 12-1 Eastern:
https://us02web.zoom.us/j/89755230924?pwd=Yp8kGYzmMhGZT7VETzzxfcqkLVH0nT.1
Meeting ID: 897 5523 0924
Passcode: 023811
The webinars are optional, not mandatory.
Speakers:
Patrick Sheehan, Whatley Kallas (Co-Lead Counsel)
Justin Wind, Brown Greer (the Settlement Notice Administrator)
Ed Gentle and Kip Benson, Gentle Turner & Benson, LLC (the Settlement Administrator)
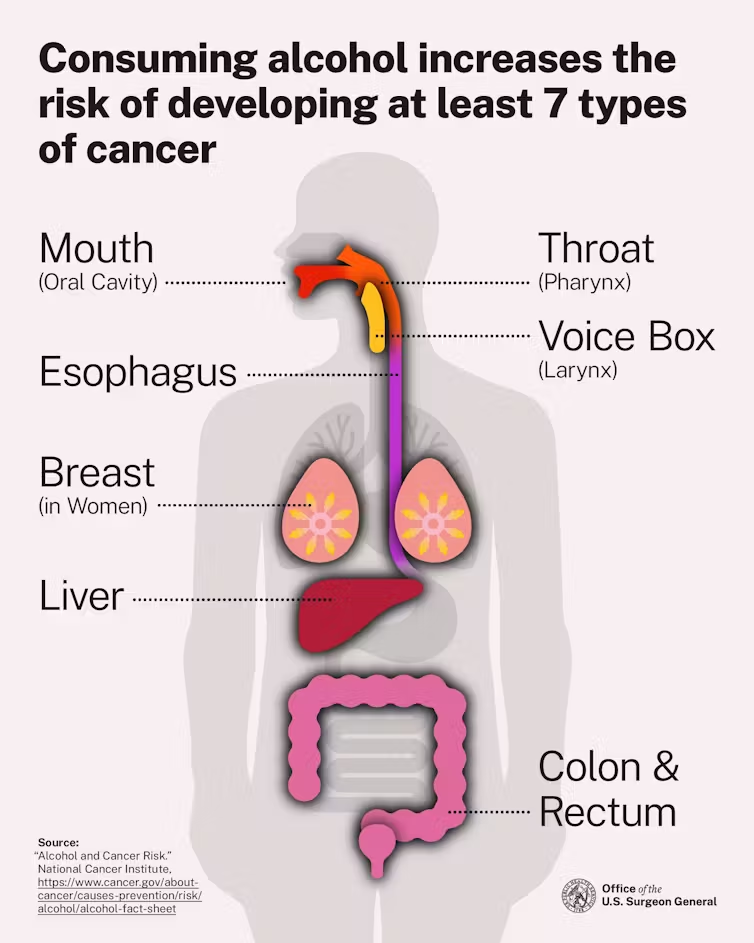
Key Takeaways in the New US Alcohol-Cancer Guidelines

Alcohol is the third-most preventable cause of cancer in the U.S, putting it just behind tobacco and obesity.
U.S. Surgeon General Dr. Vivek Murthy released a new Surgeon General Advisory on January 3, 2025, warning about the link between alcohol and cancer. This report highlighted the evidence and included a call for new cancer warning labels on alcoholic beverages.
The association between alcohol and cancer isn't new news – scientists have been trying to determine the link for decades – yet most people aren't aware of the risks and may only associate drinking with liver disease like cirrhosis. In a 2019 survey from the American Institute for Cancer Research, less than half of Americans identified alcohol as a risk factor for cancer.
As the surgeon general's report highlights, alcohol is associated with approximately 100,000 cancer cases and 20,000 cancer deaths every year, playing a role in breast, liver, colorectal, mouth, throat, esophagus and voice box cancer cases. Alcohol-induced cancer deaths outnumber alcohol-associated traffic crash fatalities every year.
Continue to full article here.

NCMS Past President Dr. Devdutta Sangvai Sworn in as Secretary of the North Carolina Department of Health and Human Services
Dr. Devdutta “Dev” Sangvai was sworn in as the new Secretary for the North Carolina Department of Health and Human Services on Sunday, January 12, 2025. Dr. Sangvai was selected by Governor Josh Stein to lead the department as the state’s 19th Secretary for Health and Human Services. The swearing-in ceremony was held at Dorothea Dix Park where the department is currently headquartered.
“I am honored to lead the Department of Health and Human Services and build on the already strong foundation toward creating a healthier North Carolina for all,” said Secretary Sangvai. “I look forward to working with the incredible team at NCDHHS and Governor Stein to ensure every North Carolinian has access to the right services to support their health, safety and well-being – no matter where they live or how much money they make.”
“Secretary Sangvai is ready for the challenge of improving the health and quality of life for children and families in North Carolina,” said Governor Josh Stein. “I look forward to working with him and the NCDHHS team to make North Carolina safer, healthier, and stronger.”
Secretary Sangvai is a family medicine physician and a professor at Duke University. He is also a member of the North Carolina Medical Board. Prior to his role with NCDHHS, he served as President of Duke Regional Hospital and President of the North Carolina Medical Society. His work has focused improving access, developing the healthcare workforce, and making care more efficient. Dr. Sangvai is the first Indian American cabinet member to serve under a North Carolina governor. See more photos of the swearing in ceremony.
Related Reading
Former NCMS President Dr. Devdutta Sangvai Picked to Lead Health and Human Services

NC Medicaid Direct: New Unit Limitations for Allergy Testing & Allergy Immunotherapy CPT Codes
Effective February 1, 2025, the CPT codes in the table below will have new unit limitations. Clinical coverage policies 1N1 Allergy Testing and 1N2 Allergy Immunotherapy are in the process of being updated to reflect this guidance. A bulletin will be published announcing the final posting of these policies.
Existing coverage will not be revoked; rather, both policies will be updated to reflect current practice standards. Please consult the relevant clinical coverage policy upon its final posting for detailed information regarding this update.
|
CPT Code |
Previous Unit Limitations |
New Unit Limitations |
|---|---|---|
| 1N1 Allergy Testing | ||
| 86003 | 36 units per year | 30 units per 365 calendar days |
| 86005 | n/a | 2 units per day up to 30 allergens per 365 calendar days |
| 95004 | 75 units per year | 80 units per 365 calendar days |
| 95017 | 30 units per date of service | 27 units per date of service |
| 95024 | 20 units per year | 30 units per 365 calendar days |
| 95027 | 20 units per year | 20 units per 365 calendar days |
| 95028 | 20 units per year | 20 units per 365 calendar days |
| 95044 | 36 units per year | 80 units per 365 calendar days |
| 95052 | n/a | 36 units per date of service |
| 95056 | n/a | 1 unit per date of service |
| 95071 | removed due to obsoletion | removed due to obsoletion |
| 1N2 – Allergy Immunotherapy | ||
| 95180 | 12 units per date of service | 6 units per date of service |
| 95145 | 1 unit per date of service | 10 units per date of service |
| 95146 | 1 unit per date of service | 10 units per date of service |
| 95147 | 1 unit per date of service | 10 units per date of service |
| 95148 | 1 unit per date of service | 10 units per date of service |
| 95149 | 1 unit per date of service | 10 units per date of service |
| 95170 | 1 unit per date of service | 10 units per date of service |
The following 10 codes will remain unchanged:
- 1N1 Allergy Testing -95018, 95027, 95028, 95070, 95076, 95079
- 1N2 Allergy Immunotherapy - 95115, 95117, 95144, 95165
This information applies to NC Medicaid Direct.

NC General Assembly Convenes, NCMS Members Sworn In
 North Carolina’s legislature opened its 2025-26 biennial assembly on Wednesday, January 8, 2025.
North Carolina’s legislature opened its 2025-26 biennial assembly on Wednesday, January 8, 2025.
Notable among the members of the General Assembly include three NC Medical Society members.
Rep. Tim Reeder, MD (R – Pitt – incumbent)
Rep. Grant Campbell, MD (R – Cabarrus, Rowan)
Sen. Mark Hollo, PA (R – Caldwell, Catawba)
The new year brings a new Speaker of the House of Representatives, Rep. Destin Hall, who succeeds Rep. Tim Moore who held the gavel from 2015 to 2025. Sen. Phil Berger will again serve as President Pro Tem of the NC Senate.
This year’s political landscape is similar to that of 2023-24 with Republican majorities in both the House and Senate and a Democrat Governor, Josh Stein. A significant difference in the upcoming 2025-26 legislative session, however, is that the Republican’s majority in General Assembly’s will not be veto-proof.
NCMS members’ photos from the January 8th House and Senate swearing-in sessions:

Both chambers will return to Raleigh on January 29th to begin this year’s business of the legislature. The 2025 session of the biennium will be the “long session,” with a clean slate of bills to be deliberated. The long session does not have a pre-set adjournment date.
The 2026 assembly will be the “short session,” a relative description since legislative sessions have no limit on duration. The second session of the biennium is typically devoted to budgetary issues and any bills that passed out of one chamber during the first session.
The NC Medical Society looks forward to working with Mr. Hollo, Dr. Campbell and Dr. Reeder and with all elected officials. NCMS physician and PA members’ involvement in the legislative process will be vital to the Society’s ability to achieve its advocacy goals, so please commit now to actively supporting those efforts. You can show your support by . . .
Signing up for the 2025 Advocacy Summit

Thank you for being involved!

NC Medicaid Releases Annual Health Disparities Report
To help identify and address health disparities, the North Carolina Department of Health and Human Services (NCDHHS) Division of Health Benefits (DHB) developed the 2022 NC Medicaid Annual Health Disparities Report, which outlines health disparities across the entire NC Medicaid beneficiary population.
The report looks at 50 quality measures and identifies health disparities across eight demographic stratifications. The results are organized into six domains: beneficiary experience, child and adolescent health, women’s health, mental health, substance use, and health care utilization. The 2022 results reveal that the domain with the largest count of identified disparities was the substance use domain, and the demographic stratifications with the highest count of identified disparities were beneficiaries who identify as having a disability and those with long-term services and support needs.
In addition to identifying health disparities, the 2022 Annual Health Disparities Report highlights programs across NC Medicaid that are working towards eliminating health inequities. This report will serve as a tool, alongside other Department and Division wide efforts, to identify areas of need and track health disparities over time.
If you have any questions about this report and its results, please email [email protected].

TODAY is the Last Day to Register for the NCMS Advanced Healthcare Leadership Program. Don't Miss this Amazing Opportunity!
Don’t Miss the Opportunity to Become a Healthcare Leader!
Register now for the AHL Program before it's too late!
Deadline to apply is Monday, January 13, 2025!
This program provides a unique leadership journey that is tailored to meet the needs of healthcare professionals at various stages in their careers. Ideally, we encourage newer/mid-career leaders and residents to enroll in the NCMS Academy for Advanced Healthcare Leaders (AHL). The program offers a distinctive curriculum that can support the leadership needs of healthcare professionals.
Why should you and your colleagues enroll in the 2025 NCMS Academy?
Research shows that the long-term benefits of leadership development programs are immeasurable.
What are some benefits of applying to an NCMS Academy for Healthcare Leadership program?
- Individual Leadership Project: Apply your newfound knowledge and skills to a real-world project of interest that drives positive change within your organization/community.
- Networking Opportunities: Connect with a community of like-minded healthcare leaders and build valuable relationships.
- Build Psychological Safety: Participate in learning sessions designed to improve self-awareness and engagement with others.
Sounds fantastic! How do I apply for the program?
Interested applicants can apply by visiting the following link: NCMS Academy for Advanced Healthcare Leaders Application
Deadline to apply is Monday, January 13, 2025.
Contact Erica Neal at [email protected] for more information.

NCMS Past President Dr. Arthur Apolinario Named Mentor of the Year
 Dr. Arthur Apolinario (image credit: Chuck Thompson | Sampson Independent)
Dr. Arthur Apolinario (image credit: Chuck Thompson | Sampson Independent)
NCMS Past President and Clinton physician Dr. Arthur Apolinario was recently named Mentor of the Year by The Center for Community-Based Primary Care Mentorship Program.
Apolinario, of Clinton Medical Clinic, earned the recognition after taking a medical student under his wing to show him what it was like to be in a small, independent practice, in a more rural setting — something future doctors aren’t taught in a classroom.
“In medical school, they don’t teach you how to run your own practice — which is a business; they don’t teach you how to be a businessman,” Apolinario said during a recent interview. They (medical schools) don’t guide you on how to set up your own practice, so this program was designed to show doctors they can be their own doctor — have their own practice.”
Apolinario said the mentorship program helps medical students better understand life in their profession in many aspects outside of the medical side of the practice. From engaging and understanding the community where they work to budgeting expenses, and employee management, all, he stressed, are often overlooked in medical school, where the focus is purely on medicine, and expecting doctors to go work for a corporate practice when they graduate.
“The program has really helped doctors learn how to be independent,” explained Apolinario. “It teaches them, through mentorship and other resources, how to deal with the legality side, talk with state officials, and manage their finances.”
Army veteran Mark Bushhouse, a former medic with the 10th Special Forces Group, in Colorado, is the mentee that Apolinario has helped under the program. Bushhouse is currently a medical student at Campbell University where he is studying to be a primary care physician.
“Through the community care program — it works in tandem through different medical societies, to connect physicians with medical students, and I put my name in the hat for that, so to speak, and that connected me with Dr. A(polinario).” said Bushhouse. ” Starting out, we did a Zoom meeting, and a couple of email exchanges, and then I had the opportunity where I spent a couple of days shadowing him in Clinton, and got a really great perspective.”
Bushhouse praised Apolinario for his hands-on approach, and the advice that was shared, stating, “He has an incredible longevity in the rural health field, and he has provided a lot of perspective and exposure to different sides of medicine through the community, business, and understanding the independent physician and rural medicine.”
The mentee said Apolinario helped him by showing him that if you find your niche in medicine, and combine that with opening, or joining a practice in the right region best fitted for your life, that is the key to a successful career. Unfortunately, many physicians never set up their own practice, opting out to work for an established practice, that is often own by a huge conglomerate, when in fact, being independent can be more rewarding.
“If you look at the total independent physicians compared to those that are employees — meaning they are not running their own practice, it’s staggering how small the number for independent doctors these days,” added Bushhouse. “It is so important to hang on to those independent practices — and besides, working as an employee for a large company, the patient doesn’t always get to interact with the practicing physician like someone can with a private practice. The connection and trust just isn’t there a lot of the times.”
Apolinario backed up that sentiment stating that physicians are not encouraged to start their own practice right out of med school. “They just don’t encourage that anymore, and it’s important to keep that going and show these young doctors that they can succeed on their own, or in a small group, just as successfully — if not more — than working for some large corporation.
“If you look at the statistics of the state, it’s shocking — about 80 percent of doctors work for other practices. We’re seeing, right here in North Carolina, an alarming number of burnout among physicians that one in 10 have even thought about suicide, if only briefly.
Apolinario’s opinion is that an independent physician seems to be happier than one working for a large company, and taking control of your own business is a big part of that difference.
“That’s the bottom line,” he added. “I’m showing younger doctors that they have a way to control their own career, such as Mark Bushhouse will do one day soon.”
Apolinario, who has been practicing in Clinton for 25 years, has enjoyed his chance to care for patients in a rural county, and get to know his patients on a more personal level.
He said now that he’s been here a quarter of a century he is starting to see the longevity of his work payoff as the babies he delivered are now adults and having children of their own, and the improvements people make in their lives, to want to live longer.
“One of the most rewarding aspects is seeing people make changes in their health,” he said, “Really reaching goals, and enjoying more time with their families. It’s not always something that can be appreciated elsewhere.”
“If anything you can see how much Dr. A really cares about his community, and it shows” Bushhouse concluded. [source]

Study: 13 Genes That Increase Risk of Osteoarthritis
A new study by researchers at the UNC Thurston Arthritis Research Center at the UNC School of Medicine has identified 13 risk genes that can increase chances for developing osteoarthritis, jumpstarting research that could lead to new, targeted treatments.
Osteoarthritis is a painful condition in which cartilage – the protective cushioning between the joints – gradually breaks down. The progressive joint disease, which affects over 32 million people in the United States, can eventually cause bone-on-bone friction, joint stiffness, and pain with every movement.
Multiple factors can influence a person’s risk of developing osteoarthritis, including injury, obesity, aging, and genetics. Recent research has found that nearly half of the risk for osteoarthritis is genetic, which has raised interest in using genetic data to develop a therapy that can stop joint tissue from degrading further.
Read the full article here.
Disaster Energy Assistance Available to 25 Counties Impacted by Hurricane Helene
The North Carolina Department of Health and Human Services’ Low Income Household Energy Assistance Program (LIHEAP) began accepting applications from the general public for the Low Income Energy Assistance Program (LIEAP) on January 2, 2025. For the 25 counties that were heavily impacted by Hurricane Helene, additional Disaster Energy Assistance funding has been appropriated by the NC General Assembly to assist households with heating costs and repairs during the colder winter months.
Beginning January 15, 2025, applications for these additional Disaster Energy Assistance funds will be accepted for eligible households residing in one of the 25 identified disaster counties during and after Hurricane Helene. These counties are Alexander, Alleghany, Ashe, Avery, Buncombe, Burke, Caldwell, Catawba, Clay, Cleveland, Gaston, Haywood, Henderson, Jackson, Lincoln, Macon, Madison, McDowell, Mitchell, Polk, Rutherford, Transylvania, Watauga, Wilkes and Yancey counties.
Households can apply for both LIEAP and the Disaster Energy Assistance funding. Households with heating services or systems that require repairs, are currently inoperable, have been disconnected or are at risk of having their services disconnected can also apply for the Disaster Energy Assistance funds.
Eligible households will receive assistance based on household circumstances and need.
“Our friends and family in western North Carolina will feel the impacts from Hurricane Helene for years to come,” said Carla West, Division Director of Human Services for Child Support, Economic Services, Aging, and Operations. “We are only midway through winter, and these funds are critical to keep residents safe and warm as they continue to recover and rebuild.”
Disaster Energy Assistance is a temporary emergency program that helps eligible households and families afford energy heating services after a natural disaster or an emergency. The program provides assistance for eligible low-income households to provide, restore or continue heating sources. Disaster Energy Assistance is available until funds are exhausted.
Individuals in one of the identified 25 disaster declared counties can apply in-person or via telephone with their local county department of social services.
To be eligible for Disaster Energy Assistance, a household must have at least one U.S. citizen or eligible non-citizen and:
- Have income equal to or less than 60% of the state median income
- Have resided in one of the identified 25 disaster declared counties listed above during Hurricane Helene and are currently residing in one of those 25 counties
- Have been impacted and suffered a loss because of Hurricane Helene
Disaster Energy Assistance was created after NCDHHS was appropriated $9 million in state funds from the NC General Assembly to help assist these disaster areas with heating related costs and repairs as a result of Hurricane Helene.
ADDITONAL LINKS OF INTEREST

Chit Chat and Chocolate Women's Health Event
Maritza Manrique-Kiniry, MD (image credit: Dosher)
Dosher Memorial Hospital will host its third annual “Chit Chat and Chocolate” Women’s Health event!
Indian Trail Meeting Hall
113 W. Moore Street
Downtown Southport
Wednesday, January 29
6 to 7 p.m.
Maritza Manrique-Kiniry, MD, a board-certified gynecologist and gynecological surgeon at Dosher Medical-Women’s Health in Southport, will share information on a variety of issues impacting women’s health and will allot time for questions.
Chef Joe Hill from the Dosher Café will serve light refreshments and health friendly chocolate bark to attendees.
This event is free of charge, and all are welcome. RSVP is suggested as space is limited. Visit dosher.org/chitchat or call Dosher Community Relations at (910) 457-3900 to reserve a seat.
Medicare Payment Cut Impact Survey Results Are In!
Medicare Payment Cut Impact Survey Results
Over the two-week period of November 14-28, 2024, the North Carolina Medical Society surveyed physicians across North Carolina regarding the 2.8% Medicare physician payment cut scheduled to take effect on January 1, 2025. Just under 500 responses were received. The initial data from the responses, summarized below, accentuates the dire situation that will result from another cut in Medicare physician payment.
The NCMS continues to advocate for a positive adjustment to Medicare payment for 2025 and has joined many state and national partner societies in an appeal to Congress to at least avert the impending cut.
Survey Results
- Are you enrolled as a Medicare provider?
Yes – 92.5%
No – 7.5%
If Medicare payment kept up with inflation, would you become a participating Medicare provider?
Yes – 11%
No - 37%
- How will another Medicare payment cut affect your practice?
| I will reduce the number of appointment slots for existing Medicare patients | 36.0 % |
| I will continue to see existing Medicare patients but not accept new Medicare patient | 23.5 % |
| I will discontinue seeing Medicare patients (unenroll) | 3.5 % |
| No change | 3.5 % |
| Unsure | 1.0 % |
| Other (see below) | 32.5 % |
“Other” / Comments:
“Will make it difficult to hire new staff to meet the increasing demands.”
“There will be longer wait times for patients to be seen.”
“Will do the best i can as a physician.”
“I will retire from practice. This is not sustainable.”
“We turn no one away but still need to keep the doors open. These consistent cuts are not making it easy.”
“Will affect payment for Medicaid”
“We are still evaluating the situation but all of the above are possible”
“Longer waits”
“I will close or leave my rural practice or have to move to a larger corporation that can handle the cuts”
“I may have to stop practicing”
“I will do the best I can, if cost too much will have to cut back on all, already 2-3 week wait”
“I will continue to take care of my Medicare patients at my personal cost”
“I will have to retire. I am just breaking even with Medicare and can no longer afford to stay in business.”
“Medicare cuts will influence private insurance reimbursements and therefore cutting ALL insurances is a risk”
“I may have to close my practice completely”
“Will make it harder to stay in business and seeing all Medicare patients”
“We are urgent care. Have yet to decide”
“It will cost the hospital that supports my practice”
“All of our MD's are taking a pay cut due to declining Medicare reimbursement”
“Affects financials significantly”
“Will greatly decrease number of slots for Medicare new patients”
“Do not have an option but will be very disheartening for future”
- What practice operation factors are impacted by Medicare payment?
| Ability to meet operational expenses (overhead, payroll) | 62.0 % |
| Ability to implement system/tech upgrades | 48.0 % |
| Ability to hire/retain staff | 47.0 % |
| Ability to recruit physicians to join the practice | 44.0 % |
- Medicare payment rates impact other payment rates (Medicaid, State Health Plan, Tricare). Will a cut in Medicare payment result in a reduction in your other patient populations . . .
Medicaid
Yes 76 %
No 24 %
State Health Plan
Yes 67 %
No 33 %
Tricare
Yes 65 %
No 35 %

N.C. Dept. of Insurance Recognized as 2024 Wellbeing First Champion, Supporting Health Worker Well-Being

In September of last year, the NC Department of Insurance revised its Uniform Credentialing Application, verifying their application is free from overly broad and invasive mental health questions. Their efforts were part of the statewide initiative, ALL IN: Caring for NC Caregivers, through the NC Clinician and Physician Retention and Well-being Consortium (NCCPRW) and the Dr. Lorna Breen Heroes’ Foundation (DLBHF).
UPDATED Uniform Credentialing Application
In 2024, HCA Healthcare, Novant Health, Sentara Health, UNC Health, and WakeMed Health & Hospitals joined NCDOI and were recognized as Wellbeing First Champions. To date, Phase 1 of ALL IN: Caring for North Carolina’s Caregivers has positively impacted 45 hospitals and supported over 14,000 credentialed health workers in North Carolina. Find additional details here.
Click here to learn more about ALL IN: Caring for NC Caregiver’s and its 3-phased approach.

![]()
Capitol Chronicle: Medicare Physician Providers and Patients Get “Grinched” by Congress - Again
Medicare Physician Providers and Patients
Get “Grinched” by Congress - Again
The waning hours of the 118th Congress offered hope but eventually became a disappointment as a fix for the Medicare physician payment cut was eliminated from the year-end funding package. The legislation enacted was a spending measure – a Continuing Resolution (CR) – to keep the federal government funded to avoid a government shutdown. The bill (H.R. 10545) passed by both chambers and signed into law by the President provides temporary funding through March 14, 2025, when Congress will again have to tackle the budgetary challenge of how it will meet the operational challenges faced by our country which depend on federal appropriations.
Among the priority issues we worked on throughout 2024 and continue to advocate for in the New Year is a fix for Medicare physician payment. The 2.83% cut that went into effect on January 1, 2025, represents the fifth year in a row that physicians have been hit with reduced payment for services, while the cost of maintaining a medical practice continues to rise.
The initial debate on the year-end CR showed promise, with not only an offset of the 2.83% cut included, but also a positive adjustment in acknowledgement of the increasing costs that medical practices are facing. Due to the costs associated with these provisions, and no designated cost offsets, this section of the bill was ultimately eliminated from the final version along with several other provisions that were in the legislation as introduced.
What now?
In our legislative and political advocacy work, there is no “off season,” so we are moving forward with our same message – with a bit more volume since the payment cut has exceeded the pain threshold for many. The 119th Congress has gaveled in, with many new faces, and we are re-engaging our incumbents while connecting with and educating our new congressional delegation members. Medicare payment reform remains a top priority, and we will not relent in our work to achieve an inflationary payment adjustment for physicians, which hospitals and other providers receive.
The first opportunity for action to retract the 2.83% cut will be in March. The House and Senate will again have to take action to avoid a budgetary shutdown of the federal government, and that funding package will be a vehicle for a Medicare payment adjustment. Be on the lookout for more information on the next concerted effort to gain payment relief and on how you can help that effort.
In the meantime, we need you on the team to help our federal advocacy efforts. We need your support . . .
Do you know your state and federal legislators? More importantly, do your legislators know you?
The NCMS can help you connect with policy makers as a constituent and advocate!
Thank you. Your engagement matters.

NCAHEC Offering Support Webinar for Primary Care Physicians

SPECIAL WEBINAR
Collaborative Care Management Capacity Building Fund
Tuesday, January 28 | 12:15-1 p.m.
The NC General Assembly has earmarked $5 million for capacity building for Medicaid-enrolled primary care practices across the state to adopt Collaborative Care Management (CoCM). NCDHHS is contracting with CCNC to manage the program in partnership with NC AHEC’s Practice Support coaching.
CoCM is an evidence-based behavioral health integration model designed to support primary care clinicians in assessing and treating patients with mild to moderate behavioral health conditions. An evidence-based model shown to be more effective than usual care, CoCM improves patient outcomes, increases satisfaction for both patients and providers, and reduces healthcare costs and the stigma related to mental health and substance use disorders.
The capacity building fund has a maximum award of $50,000 per practice. A primary care practice entity applying on behalf of multiple primary care practice sites may receive a maximum of three awards per entity (covering a maximum of 9 sites). Each clinic site may be eligible to receive awards of $50,000 to begin a CoCM model in-house. Additionally, $30,000 is available for practices to expand an existing in-house CoCM model and $20,000 is available to practice sites meeting Phase 1 eligibility, but planning to outsource staffing to a third-party, turn-key company.
Please join for a webinar on January 28 from 12:15-1 p.m. for a review on the new funding and an opportunity to ask questions.
Webinar learning objectives:
- Provide an overview of the Collaborative Care Management Capacity Building Fund award opportunities
- Define eligibility criteria for practice entities/sites
- Describe the application process
For more information about this program, visit CCNC's webpage on CoCM capacity building fund.

Register Now for 2025 NC Summit on Reducing Overdose
2025 NC Summit on Reducing Overdose
March 18, 2025 - March 20, 2025
Raleigh Convention Center
Reserve Your Seat
March 18-20, 2025 • Raleigh Convention Center, Raleigh, NC
The NCACC’s 2025 Summit on Reducing Overdose brings together local government leaders, subject matter experts, service providers, community partners and people with lived experience working in crucial areas of the opioid overdose crisis, including in prevention, early intervention, harm reduction, treatment and recovery efforts. This event will provide a space for county commissioners and staff and their community partners to participate in and learn from experts and each other over a two-and-a-half day conference in Wake County.
Schedule
- Tuesday, March 18, 2025, from 1-5 p.m.
- Reception/Community Service Activity from 5-7 p.m.
- Wednesday, March 19, 2025, from 8 a.m. – 5 p.m.
- Reception/Evening Program from 5-8 p.m.
- Thursday, March 20, 2025, from 8 a.m. – 3 p.m.
Hotel and Travel Information
The Summit will take place at the Raleigh Convention Center. The nearby hotel options for self-booking are listed here.
Information on how to get to the Summit location in Raleigh, NC is listed below:
- Planes: Raleigh-Durham Airport (RDU) is the closest airport. RDU is an 18-minute drive to and from the Raleigh Convention Center.
- Trains: Raleigh Union Station (RGH) serves as a stop for the Carolinian and Piedmont Amtrak trains. RGH is about a 12-minute walk to and from the Raleigh Convention Center.
- Automobiles: To find driving directions, enter in the Raleigh Convention Center address: 500 South Salisbury Street, Raleigh, NC 27601. Parking is available at the Raleigh Convention Center.
Registration Deadline
Deadline to register for the Summit is Tuesday, March 11, 2025, by 11:59 p.m.
Payment and Cancellations
Payment by credit card (Visa or Mastercard) is required at the time of registration. If an alternate payment method is needed, please email [email protected]. Please note, there will be a $40 administrative fee for any cancellations. Any cancellations made after March 11, 2025, will not be refunded.
All attendees and participants in NCACC meetings and events are required to abide by NCACC’s Event Code of Conduct.
Note: If you have any questions about this event registration, please email [email protected].

NCDHHS Offers Tips and Vaccine Recommendations for Providers Caring for Pregnant Persons

Every Mother, Every Baby, Every Time Tip Sheet
NCDHHS / Division of Public Health has produced an infographic “Every Mother, Every Baby, Every Time,” which presents conversation tips and vaccine recommendations for providers caring for pregnant persons. Immunizations can help protect women and their babies against diseases including flu, COVID-19, RSV, and pertussis. Making strong vaccine recommendations, especially during respiratory season and while the state is experiencing an increase in pertussis cases, is an important way providers can help prevent disease.
Cases of pertussis have been on the rise nationally and in 2024 the North Carolina Department of Health and Human Services (NC DHHS) is reporting one of the highest counts of pertussis cases in decades. As of January 6, 2025, state public health officials had recorded 784 cases, including 73 cases in infants. Cases are slightly more concentrated in the western region, but cases have been reported across the state, including 18 reported outbreaks.
Infants have the highest incidence rates in North Carolina and are at greatest risk of hospitalizations and death from pertussis. Approximately half (51%) of all cases have occurred in individuals that were up to date with their age-appropriate pertussis-containing vaccine. More than half (56%) of cases in infants occurred in infants with no record of a maternal Tdap vaccine.
If your office is interested in accessing the North Carolina Immunization Registry to view and record vaccine administrations, please contact the North Carolina Immunization Program’s Help Desk at 1-877-873-6247.

Do New CMS Rules on Prior Auth Go Far Enough? Some Physicians Say No!
Do the new CMS rules on prior authorization go far enough?
— No, say some physicians and advocacy groups.
(MedPage Today, Joyce Frieden, Washington Editor) -- The new CMS regulations on prior authorization have been heralded as a big step forward in reducing administrative burdens on physicians, but some people think it doesn't go far enough.
The CMS regulations, which were issued last January, require federally regulated health plans to "improve the electronic exchange of health information and prior authorization processes for medical items and services," according to a CMS press release. For example, starting next year, affected plans must send prior authorization decisions within 72 hours for urgent requests and 7 calendar days for non-urgent requests. The rule also requires all impacted payers to include a specific reason for denying a prior authorization request, and payers must publicly report prior authorization metrics.
But Alex Shteynshlyuger, MD, a New York City urologist, noted in a phone interview that the regulation is limited to Medicare Advantage (MA) plans, Medicaid HMOs, and some plans on the Affordable Care Act's insurance exchanges, though it also includes plans in the Children's Health Insurance Program. In addition, the prior authorization requirements only apply to requests from physicians who are in the MA plan's network, he said.
That excludes providers like him, who aren't in an MA plan but do accept traditional Medicare and also provide care to MA enrollees who have out-of-network benefits. "They are receiving claims from me; they're receiving medical records from me. I've already been verified by Medicare, right?" said Shteynshlyuger, who brought up some of his concerns at the interim meeting of the American Medical Association (AMA) last November. "[But] CMS comes in and says, 'These providers are not vetted enough,' even though we are sending claims to [Medicare] for the same patients and receiving payments from them ... This is irrational logic by CMS to try to create impediments for physicians who do not want to sign unfair contracts from insurance companies."
Shteynshlyuger also is unhappy that CMS is instituting "enforcement discretion" -- meaning that the agency generally won't be enforcing the rule -- for a provision of the Health Insurance Portability and Accountability Act of 1996 (HIPAA), known as X12, that requires health plans to implement electronic transactions for prior authorization. "The enforcement discretion as issued is overly broad, lacks any rational basis, and lacks reasonable justification," he wrote in a December 29 letter to the agency. "The decision to issue a broad discretion is arbitrary and capricious. CMS lacks legal authority to issue such regulatory guidance and lacks authority to suspend enforcement without going through the [Administrative Procedures Act] required notice and comment period." Shteynshlyuger said he has not yet heard back from CMS about his letter.
Asked about some of Shteynshlyuger's concerns, a CMS spokesperson said in an email that it is not enforcing the HIPAA rule as long as the affected plans instead use a standard programming interface that allows for electronic prior authorizations. "Covered entities may separately continue to make an X12 prior authorization process available to providers," the spokesperson said, adding that "HHS will continue to evaluate the HIPAA prior authorization transaction standards for future rulemaking."
In addition, the spokesperson said, "To encourage providers to adopt electronic prior authorization processes, this final rule also adds a new measure for Merit-based Incentive Payment System (MIPS)-eligible clinicians," as well as hospitals, related to using electronic prior authorizations.
The AMA agrees that prior authorization is still a big problem, AMA President Bruce Scott, MD, said in a phone interview that was conducted with a press person present. "I think there's a growing awareness across health systems that [prior authorization] is overused, unjustified, and needs to be right-sized," he said. "Patients are becoming increasingly aware of this overused blunt cost-control process by insurance companies. As a result, there is anger that's building and frustration among physicians that has grown as well."
The "partial fix" that CMS issued last January "didn't go far enough," Scott said. And he is concerned that even the CMS regulations will have limited effectiveness because of the Supreme Court's Chevron decision, issued last July, which overturned a 1984 ruling saying that whenever a dispute emerges over regulating an ambiguous law, judges should defer to the interpretation of federal agencies, assuming those interpretations are reasonable.
In the wake of the Chevron ruling, the AMA is anxious to see the prior authorization regulations be codified by Congress so they aren't in danger of being challenged. The association therefore is supporting the Improving Seniors' Timely Access to Care Act, which would cement the CMS regulations into law. That bill, which had bipartisan support in the House and Senate, appeared to be on the brink of passage, but was ultimately left out of the budget deal that Congress passed at the end of last year.
"The frustration was that this was a bipartisan, bicameral bill that was in the [budget deal] that would have fixed [prior authorization] in many ways, and instead, it gets cut," Scott said. "We're not pushing for something radical here. We're saying we need to right-size this. We're pushing for transparency, we're pushing for efficiency and for communications that are electronically linked so we don't have to use fax machines."
Shteynshlyuger, who is an AMA member, said he is not a fan of the bill because it lacks an enforcement mechanism. "The original bill had enforcement requirements," but those were removed in order to bring the cost of the bill down and thus increase its chances of passage, he said. "Unfortunately, organized medicine has been either misled as to what the bill says, or is complicit. I requested that the AMA withdraw their support for this bill in Congress."
Instead, the House and Senate "should issue comprehensive rules or prior authorizations that apply to every health plan," including employer-sponsored plans, he said. "We cannot live another day under the disastrous systems we have today." Currently, the Labor Department is looking at whether to regulate prior authorization in employer-sponsored health insurance plans; the AMA testified about the issue at a September 2024 meeting of the department's Employee Retirement Income Security Act Advisory Council.
Another complaint about the CMS rules is that they don't apply to pharmacy services, or to prior authorization for drugs administered inside physician offices. CMS said it is developing a proposed rule to streamline prior authorization for drugs covered under federally regulated plans, and that it plans to issue the proposed rule in March.