

Thousands of American Youth Living with Inflammatory Bowel Disease
A study published in Gastroenterology provides the most comprehensive assessment to date of pediatric inflammatory bowel disease (IBD) prevalence in the United States.
The research, led by investigators from the Crohn's & Colitis Foundation, University of North Carolina at Chapel Hill, and the University of Pennsylvania, estimates that more than 100,000 American youth under the age of 20 live with IBD. The study illustrates that the prevalence of pediatric IBD in the U.S. continues to increase and is among the highest worldwide.
This landmark study analyzed data from two commercial insurance claims datasets (Optum's Clinformatics Data Mart database and Carelon Research's Health care Integrated Research Database) and Medicaid data from five states (Florida, New York, Pennsylvania, Ohio, and California), providing a nationally representative picture of physician-diagnosed pediatric IBD across the country.
The researchers utilized a validated combination of medical diagnoses and prescription medications to identify IBD cases, and calculated age-, sex-, and race-specific estimates of IBD prevalence. These estimates were then standardized to the 2020 United States Census to generate national prevalence estimates. The study found an increase of about 22% for Crohn's disease and 29% for ulcerative colitis in the pediatric population compared to 2009 prevalence data.
Continue to full article here.

Preparing for Your Thanksgiving Feast? Put Food Safety at the Top of Your List!

The Holidays are a Time for the Three F's: Family, Feasts, and Fun!
Whether you’re cooking up a classic turkey dinner, baking mouthwatering desserts, or preparing that famous side dish, food safety should be a priority! As you start to gather your ingredients, be sure to check the FDA’s Recalls, Market Withdrawals, & Safety Alerts list.
Around Thanksgiving and Christmas, rates of foodborne illness tend to rise, often due to the increased handling of raw meats, dairy products, and the large volumes of food being prepared and shared. According to the CDC, 1 in 6 Americans gets sick from foodborne illnesses each year. Though most cases are mild, serious illnesses can lead to hospitalizations or even death.
Common Foodborne Illnesses during the holidays:
- Salmonella: One of the most common culprits during the holidays, particularly from raw poultry.
- E. coli: Found in undercooked meat, especially ground beef, E. coli bacteria causes serious stomach cramps and diarrhea. During the holiday season, the USDA noted that over 40% of E. coli outbreaks occurred in December and January.
- Listeria: Linked to dairy products, deli meats, and even fresh produce, Listeria is particularly dangerous for pregnant women and can lead to miscarriage or severe health complications. The CDC reports that Listeria outbreaks are more likely to be reported in the colder months when foods like cheese and deli meats are more commonly consumed.
Tips for Holiday Food Safety:
- Pay attention to recalls
- Thoroughly wash hands and utensils
- Cook to the proper temperature
- Refrigerate leftovers (refrigerate within two hours of cooking)

Mobile Outreach Unit Delivering Essential Care to Uninsured
Meeting patients where they are: That’s the simple but impactful mission behind UNC Health Johnston’s Mobile Outreach Unit.
The bus is equipped with various medical equipment, an exam table and a consultation area.
Leah Johnson works as UNC Health Johnston’s community outreach coordinator. She explained the goal of the mobile unit is to serve as the first point of care while connecting patients to primary care physicians and long-term resources.
“We work with the patient from the moment we’re creating their medical chart in our electronic system, to getting them registered for their appointment, connecting them with a physician, helping them figure out how to go to the hospital to get their labs drawn, helping them pay for that and helping them pay for medication if they need it,” shared Johnson.
Registrations for most clinics and screenings are not required.
Many of the walk-in patients Johnson sees are uninsured.
“It feels like all the time we run into diabetics and people with high blood pressure who know they have a diagnosis, who have previously been on medication, but because they’re uninsured they have let their health fall to the wayside,” said Johnson.
The Mobile Outreach Unit holds five urgent care clinics each month spread throughout Johnston County. Clinics are often held on weekends or after hours on weekdays to help with accessibility.
Clinics are open to patients between 6 months and 65 years of age.
Some screenings have additional requirements for eligibility, for example lung cancer screenings through the Mobile Outreach Unit require patients to have a long-term history of smoking.
Read the full article here.

It's 'Easier for You' to Renew Your 2025 NCMS Membership
The immediate crisis caused by Hurricane Helene in Western North Carolina has subsided. Now, the long journey to full recovery is beginning.
Included on your 2025 invoice is a spot to Round Up When You Renew! The money raised will support your colleagues as they re-build, re-open, and start to care for patients again.
Also, we’ve made it Easier for You to renew your 2025 state, county, and NCMS managed specialty society dues … all on one convenient invoice.
Look for your 2025 Membership Dues Invoice in your inbox or renew online now — and remember “Round Up and Renew” and it’s “Easier for You.”

FDA Approves Revuforj to Treat a Genetic Form of Leukemia
image credit: pharmaphorum
Just three days after Syndax Pharmaceuticals revealed data from a trial of revumenib in one indication of acute leukemia which chilled investors, the FDA has approved the small molecule in another indication of the disease.
On Friday, the U.S. regulator signed off on Revuforj as the first menin inhibitor to treat a genetic type of leukemia called lysine methyltransferase 2A (KMT2A). The nod applies to patients one year and older with relapsed or refractory leukemias who have rearrangements of the KMT2A gene.
The approval came six weeks ahead of its target date and is the second FDA new drug endorsement for Syndax in the last three months. In August, Syndax and its commercial partner Incyte earned a thumbs up for Niktimvo (axatilimab), a CSF-1R inhibitor to treat chronic graft-versus-host disease (cGVHD) in patients who’ve failed at least two prior lines of systemic therapy.
Continue to full article here.

Reminder: Disaster Relief Applications for Health Care Professionals Not Currently Enrolled as an NC Medicaid Provider
The NC Department of Health and Human Services is committed to ensuring continued access to care for NC Medicaid beneficiaries, as well as reimbursement to qualified providers for services rendered, in good faith, throughout the period of impacts from Hurricane Helene, retroactively from Sept. 25, 2024, through Dec. 31, 2024, (unless otherwise communicated by DHHS).
- The Centers for Medicare & Medicaid Services (CMS) granted approval effective October 1, 2024, for DHHS to implement a temporary, expedited enrollment process for health care professionals to become an NC Medicaid provider due to a natural disaster. This process is not for providers who regularly see NC Medicaid beneficiaries.
Health care professionals who will be rendering services to NC Medicaid beneficiaries due to Hurricane Helene can complete and submit an application through the NCTracks Provider Portal. Please refer to the disaster provider enrollment job aid Disaster Relief Provider Enrollment Application Job Aid (PRV703) located under Quick Links on the NCTracks Provider Enrollment home page for necessary instructions to complete the temporary disaster provider enrollment application. Be sure to review the job aid before starting to complete the application, as several preliminary steps are necessary.
Providers must indicate the application is for Disaster Relief by answering “Yes” to the Disaster Relief enrollment question on the Online Application page of the application.
Note: This is not for providers who see NC Medicaid beneficiaries on a regular basis.
Please review North Carolina Medicaid Provider Enrollment Disaster Relief and Waiver or Modification of Requirements Under Section 1135 of the Social Security Act from the Secretary of Health and Human Services for additional information.
Information about Governor Cooper’s Declaration of a State of Emergency can be found at Governor Cooper Declares State of Emergency Ahead of Hurricane Helene.
Contact:
- NCTracks Call Center: 800-688-6696
- Provider Ombudsman: 866-304-7062, [email protected]

Don't Miss Thursday's Medicaid Managed Care Fireside Chat
Medicaid Managed Care Fireside Chat
Thursday, November 21
12:00 p.m. - 1:00 p.m.
Please join this month's Fireside Chat on November 21, hosted by Dr. Janelle White, Chief Medical Officer of Medicaid, Medicaid colleagues and CEOs from Standard Plans and Tailored Plans.
Topics will include:
- Hurricane Helene response and recovery efforts
- Results from the 2023 Consumer Assessment of Healthcare Providers and Systems
- Medical Clinical Policy Updates
- Pharmacy Updates
- Collaborative Care Capacity Building Program (CoCM)
- Community Alternatives Program (CAP) Referral Process for Children and Disabled Adults


Save the Date: 2nd Annual CoCM Behavioral Health Care Manager Summit

2nd Annual CoCM Behavioral Health Care Manager Summit
May 16, 2025
Conference Center at GTCC | Colfax, NC
Mark your calendar for the 2nd Annual Collaborative Care Model (CoCM) Behavioral Health Care Manager (BHCM) Summit, presented jointly by NC AHEC and Southern Regional AHEC. Explore the pivotal role of BHCMs in CoCM and their significant impact.
This summit will feature esteemed national and state CoCM experts, including representatives from the AIMS Center at the University of Washington. Attendees will benefit from insightful presentations by experienced CoCM BHCMs and integrated behavioral health Subject Matter Experts.
Don't miss out on this invaluable training opportunity! Registration details will be available soon.
Collaborative Care Model: Problem-Solving Therapy Training
COLLABORATIVE CARE MODEL (CoCM)
Problem-Solving Therapy (PST) Training
December 2 | 9 a.m.-4 p.m.
Please join on December 2 from 9 a.m. to 4 p.m. at Southern Regional AHEC in Fayetteville to empower your practice with Problem Solving Therapy (PST).
PST is an evidence-based model that employs short interventions to help individuals develop effective coping skills to manage life’s challenges. This six-hour skills-building workshop will give Behavioral Health Care Managers working in Primary Care and Specialty Care settings an understanding of the fundamental principles of Problem-Solving Therapy.
Speaker: Annie McGuire, MS, LMHC, MHA Clinical Trainer & Practice Coach, AIMS Center, University of Washington
Objectives:
• Identify the steps involved in the PST model.
• Explain the role of PST in Collaborative Care Model.
• Describe how PST can improve patient outcomes.
• Demonstrate the application of PST techniques in clinical scenarios.
• Use PST strategies to address common patient issues.
• Evaluate the effectiveness of PST interventions in practice.
• Critique different PST techniques based on patient outcomes.
• Develop personalized PST plans for patients.
• Design innovative solutions to integrate PST into collaborative care.
MedBoard Matters Podcast: NC DHHS’s Response to Hurricane Helene
The North Carolina Medical Board's Jean Fisher Brinkley talks with State Health Director Dr. Betsey Tilson about all of the things NC DHHS has been doing to safeguard the health and safety of people impacted by Hurricane Helene, how they are helping licensees safely continue to practice, and more.
Jean Fisher Brinkley
Communications Director, North Carolina Medical Board

Jean Fisher Brinkley is NCMB’s Communications Director, a role that involves developing and overseeing production of communications materials and strategies needed to enhance public and professional awareness and understanding of the Board and its mission. She joined NCMB in 2008, after an 11-year career in newspaper journalism, most of it dedicated to reporting on medicine, health policy and the business aspects of health care.
Brinkley earned a bachelor’s degree in English from Mills College in Oakland, CA, and a master’s degree in journalism from the University of California, Berkeley. She lives in Raleigh with her husband and two daughters.
You can reach Jean at [email protected]
Dr. Betsey Tilson
State Health Director and NC DHHS Chief Medical Officer

Elizabeth Tilson serves North Carolina as the State Health Director and the Chief Medical Officer for the Department of Health and Human Services. In this role, she promotes public health and prevention activities, as well as provides guidance and oversight on a variety of cross-Departmental issues including the COVID-19 Pandemic Response, the Opioid Epidemic, Early Childhood, Medicaid Transformation, and Healthy Opportunities.
Prior roles include serving as the Medical Director of Community Care of Wake and Johnston Counties, Chief Network Medical Director for Community Care of North Carolina, and Assistant Consulting Professor and Cancer Control Specialist with Duke University Medical Center. Dr. Tilson practiced primary care pediatrics for 26 years and has been active in leadership roles in many local, state, and national pediatric, public health and preventive medicine organizations.
Dr. Tilson is a graduate of Dartmouth College (BA), Johns Hopkins University School of Medicine (MD), and the University of North Carolina – Chapel Hill (MPH). She completed Residencies and is board certified in both Pediatrics and General Preventive Medicine/Public Health.
URGENT: Impending Medicare Physician Payment Cut Is Looming
U R G E N T
Impending Medicare Physician Payment Cuts
Impact Survey
For four consecutive years, Medicare providers have experienced annual payment cuts, while the costs of maintaining a practice and healthcare facilities have increased annually. Another 2.8% payment cut is scheduled for 2025, and practice costs are projected to increase by 3.56% over the next year.
The North Carolina Medical Society continues to engage with members of Congress to find a solution to the growing crisis resulting from these devastating cuts, and we urgently need your assistance in that effort. Help us make our outreach on Capitol Hill more impactful by sharing information on how previous and anticipated cuts have and will affect your practice and your patients.
Please respond to this survey by November 22, 2024. Please also help this effort by circulating this notice and survey with your colleagues. The more responses we receive, the stronger our message.
NOTE: At the end of the survey, we ask for your contact information. That information will not be shared in any distribution of the survey results without your explicit permission. We need practice/contact information to avoid duplicate entries of responses, since the survey notice will be sent through multiple channels and could generate more than one reply from a practice. We especially need home addresses, which is how individuals' members of Congress are identified. This will enable us to quantify and qualify the impact of Medicare cuts geographically. We respect the confidentiality of your information.


ALL IN: First Round of Wellbeing First Champion Award Recipients Recognized!
At the North Carolina Medical Society’s LEAD Conference Gala, hospitals and health systems that completed Phase 1 of ALL IN: Caring for North Carolina’s Caregivers initiative were honored on-stage. The Dr. Lorna Breen Heroes’ Foundation CEO Corey Feist, JD, MBA and CMO Stefanie Simmons, MD, FACEP, along with NCMS CEO Chip Baggett, JD, presented these organizations with the Wellbeing First Champion badge.
![]()

This year, the North Carolina Clinician and Physician Retention and Well-being (NCCPRW) Consortium and the Dr. Lorna Breen Heroes’ Foundation (DLBHF) launched their partnership with the ALL IN: C4NCC initiative, beginning with Phase 1 – Breaking Down Barriers to Help-Seeking. To qualify for the Wellbeing First Champion badge, hospitals and health systems must remove invasive and stigmatizing mental health language from credentialing applications, addendums, and peer review forms.
Since its launch in April, ALL IN: C4NCC is proud to recognize the following health systems and organizations as Wellbeing First Champions, celebrating their commitment to protecting and prioritizing health worker well-being.

 Tameka Peterson, Vice President, Chief Provider Experience Officer for Credentialing & Medical Staff Operations accepted the award
Tameka Peterson, Vice President, Chief Provider Experience Officer for Credentialing & Medical Staff Operations accepted the award


Nadia Charguia, MD, Executive Medical Director of the Well-being Program at
UNC Health and UNC School of Medicine accepted the award.
![]()

Michelle McMoon, PA-C, PhD, Director of Education and Professional Development and Chair of the WakeMed Physicians Practices
Well-being subcommittee and Susan Force, Director of Medical Staff Services accepted the award.

 Mike Causey, Commissioner of Insurance accepted the award.
Mike Causey, Commissioner of Insurance accepted the award.
Recognized, but not present.


North Carolina is inviting all remaining hospitals, health systems, and practices that credential licensed health workers to go “ALL IN” and join the efforts of NCCPRW and DLBHF. Together, we’re taking steps to improve workplace policies and practices that reduce burnout, normalize help-seeking, and strengthen professional well-being – accelerating impact to improve health workers’ well-being and mental health.

Click here to learn more about ALL IN: Caring for NC Caregiver’s and its 3-phased approach.

Amazing Turnout for NCMS Social in Cary!

The final NCMS Social of 2024 draws big crowd despite bad weather!
CARY -- The final NCMS Social or Regional Meeting is in the books and it was fantastic! This time it was fun for members and guest, but also families! A big thank you to Dr. Alan Rosenbaum for bringing his child (who was the star of the event)!
The NCMS Director of Membership and Engagement, Toni Hill, says "Despite the nasty weather, we had an amazing turnout of members and non members. It was a great night of connecting our community, across specialties! It was also nice to have some kids involved because we love seeing our members' families too!"

Look for our first Regional Meeting in the Fayetteville area in January and our first NCMS Social in Raleigh in February. Details coming soon!
NC Radiological Society Virtual Breast Imaging Review Course (Jan. 17-19, 2025)
Date/Time
Date(s) - January 17, 2025 - January 19, 2025
Time TBA
Save the date for the NC Radiological Society Virtual Breast Imaging Review Course!
January 17-19, 2025 - Virtual
Manteo Healthcare Task Force Talks Project VBOT, Applauds NCMS Work in Outer Banks

Town of Manteo considers using the NCMS Foundation Project VBOT
The Manteo Healthcare Task Force met with NCMS's Franklin Walker to talk about the Virtual Based Opioid Treatment (VBOT) Program. At the meeting, the Mayor of Manteo thanked the NCMS Foundation and Walker for helping set up the Outer Banks Medical Group, the NCMS Preceptor Hub formed in partnership with Manteo Community Health in Manteo, Engelhard, and Ocracoke.
The conversation, however, focused on how to bring virtual care to area residents. The program would allow law enforcement or recovery programs to connect patients with virtual counselling, mail-in drug screenings, and help eliminate long commutes to treatment facilities.
The mission of Project VBOT is to facilitate patient access to treatment, contain treatment costs, empower clinicians, deliver advanced methodology, and connect with communities.
Walker said after the meeting that "It is three or four hours for a behavioral health provider to drive down here. With our model that won't happen. A person in treatment in our model can be at home or be in their car and we can see them over telehealth."
Manteo and the Task Force are in early discussions with the NCMS about joining the program.
For more on Project VBOT click below.
![]()
NC Receives National Award for Medicaid Expansion
NC Medicaid is the recipient of the National Association of Medicaid Directors’ 2024 Spotlight Award.
RALEIGH -- NC Medicaid is the recipient of the National Association of Medicaid Directors’ 2024 Spotlight Award. This recognition for the North Carolina Department of Health and Human Services comes as more than 570,000 people have enrolled in Medicaid expansion in the 11 months since its Dec. 1, 2023, launch. The record enrollment in year one is almost the total 600,000 that were estimated to enroll in Medicaid expansion over two years.
"We never gave up on making sure more North Carolinians got health insurance through Medicaid Expansion," said Governor Roy Cooper. "Now, more of our neighbors, friends and loved ones can see a doctor, get preventative care, manage chronic conditions and get life-saving prescriptions without the burden of high premiums or co-pays."
The award from NAMD attributes the record enrollment in part to NCDHHS’ extensive outreach efforts that included a collaboration with community partners. More than 215 partners across all 100 counties in the state including local organizations, health care providers, business leaders, community advocates and elected officials are all participating in sharing information about Medicaid expansion with their communities ensuring more North Carolinians can get health care coverage through Medicaid.
Since launch, these community-centered approaches led to more than 270,000 people being enrolled the first day of Medicaid expansion and more than 570,000 enrolled as of Nov. 14, 2024. New Medicaid enrollees have filled more than 3.4 million prescriptions for heart health, diabetes, seizures and other illnesses. Medicaid has also covered more than $53 million in claims for dental services since Medicaid expansion began.
"We got Medicaid expansion done — and we got it done well — with the help of our state and community partners who worked tirelessly to make it easier and more accessible for people to apply," said NC Health and Human Services Secretary Kody H. Kinsley. "Nearly 600,0000 people are already seeing the positive impact and life-saving care made possible by Medicaid expansion."
North Carolina’s outreach efforts include a dedicated website and Community Engagement Toolkit that enabled organizations to tailor Medicaid messaging for their specific communities. Partners can customize materials in multiple languages including Arabic, Spanish and Swahili, all while maintaining crucial information about enrollment processes through ePass or county departments of social services.
Additionally, the Medicaid Ambassador initiative empowered North Carolinians to help their neighbors navigate the Medicaid system. This volunteer program provides comprehensive training and resources, allowing community members to confidently guide others through the application process.
"North Carolina's approach demonstrates how centering community voices can transform program implementation," said NAMD Executive Director Kate McEvoy, "their innovative partnership model breaks new ground."
To learn more about or apply for NC Medicaid, visit Medicaid.nc.gov and read the Medicaid expansion FAQs.

Make Plans Now! Join NCMS for 2025 National Advocacy Conference

Registration is open!
Make your plans today to join us in Washington, DC for the
AMA’s 2025 National Advocacy Conference

2025 National Advocacy Conference
February 10-12, 2025 / Washington, DC
Use these links to Register and
to secure your Accommodations.
The 2025 NAC will address urgent health policy issues
Impacting the medical profession and patients like
Medicare payment reform
Workforce challenges
Prior Authorization
Make plans today to be part of our North Carolina team
Headed to Capitol Hill in February. Your support matters!
If you have more questions, contact Alan Skipper, NCMS VP External Affairs, [email protected]
Do you know your state and federal legislators? More importantly, do your legislators know you?
The NCMS can help you connect with policy makers as a constituent and advocate!
Shine-A-Light on Lung Cancer Event is Tuesday. Make Plans to Attend Today!
Lung cancer continues to be one of the most common cancers in America, and it is the leading cause of cancer deaths annually.
The American Cancer Society estimates about 234,580 new cases of lung cancer will be diagnosed in 2024, while about 125,000 will die from the disease. These numbers are more than colon, breast and prostate cancers combined.
In partnership with GO2 Foundation for Lung Cancer, FirstHealth will host its annual Shine-A-Light event at 5:30 p.m. on November 19 at the FirstHealth Cancer Center located at 135 Page Road North, Pinehurst, N.C.
The event is free and open to the public and will include a presentation about clinical trials at FirstHealth. The research treatment opportunities at FirstHealth are part of the same research treatment opportunities that you would find at the country’s leading academic hospitals.
Event attendees will also be able to take part in a lighting ceremony.
FirstHealth’s event will be one of more than 200 similar events held across the country during November, which is Lung Cancer Awareness Month.
For more information or to register for FirstHealth’s Shine a Light on Lung Cancer event or to register, call 800-213-3284. For more information on cancer services provided by FirstHealth of the Carolinas, visit nccancercare.org. [source]

Don't Miss this Leadership Opportunity! Deadline for Applications is November 30, 2024.
Don’t Miss the Opportunity to Become a Healthcare Leader!
Register for a Leadership Program Today
Deadline to apply is November 30, 2024
The NCMS Kanof Institute for Physician Leaders presents the Academy for Advanced Healthcare Leaders and the Academy for Executive Healthcare Leaders. We are excited to announce that both programs are currently accepting applications for 2025.
Each program provides a unique leadership journey that is tailored to meet the needs of healthcare professionals at various stages in their careers. Ideally, we encourage newer/mid-career leaders and residents to enroll in the NCMS Academy for Advanced Healthcare Leaders (AHL) and more senior-level healthcare clinicians and administrators to enroll in the NCMS Academy for Executive Healthcare Leaders (EHL). Both programs offer a distinctive curriculum that can support the leadership needs of healthcare professionals.
Note: Both programs are CME eligible.
Why you and your colleagues should enroll in the 2025 NCMS Academy
Research shows that the long-term benefits of leadership development programs are immeasurable. Here are a few benefits of applying to an NCMS Academy for Healthcare Leadership program:
- Individual Leadership Project: Apply your newfound knowledge and skills to a real-world project of interest that drives positive change within your organization/community.
- Networking Opportunities: Connect with a community of like-minded healthcare leaders and build valuable relationships.
- Build Psychological Safety: Participate in learning sessions designed to improve self-awareness and engagement with others.

- 360-Degree Leadership Assessment: Gain a deeper understanding of your strengths, weaknesses, and blind spots through a comprehensive 360-degree assessment.
- Personalized 1:1 Executive Coaching: Work closely with a seasoned executive coach to develop a personalized leadership development plan to address specific challenges.
- Experiential Change Initiative Project: Develop and implement a change initiative project that can improve outcomes for patients, organizations, and healthcare systems.
Apply Today!
Interested applicants can apply by visiting the following links, respectively:
NCMS Academy for Advanced Healthcare Leaders Application
NCMS Academy for Executive Healthcare Leaders Application
Deadline to apply for each program is November 30, 2024.
Contact Erica Neal at [email protected] for more information.

CDC: Black Infant Mortality Rate More Than Double Rate Among White Infants
Black infants died at a rate of 10.9 deaths per 1,000 live births, the CDC said.
(ABC News, Mary Kekatos and Dr. Harika Rayala) -- Infant mortality rates remained relatively unchanged from 2022 to 2023, but racial and ethnic disparities still persist, new provisional federal data released early Thursday finds.
The U.S. provisional infant mortality rate in 2023 was 5.61 infant deaths per 1,000 live births, unchanged from the 2022 rate, according to a report from the Centers for Disease Control and Prevention's National Center for Health Statistics (NCHS).
The report also found that infants born to Black mothers still died at much higher rates than those born to white and Asian mothers -- more than double the rate of white infant mortality, according to the CDC.
Additionally, changes in the neonatal mortality rate from 3.59 deaths per 1,000 live births in 2022 to 3.65 deaths per 1,000 live births in 2023, and the postneonatal mortality rate from 2.02 deaths per 1,000 live births to 1.96 deaths per 1,000 live births from 2022 to 2023 were not seen as statistically significant, the report's authors said.
Neonatal refers to the first four weeks of an infant's life and postneonatal refers to the period between 28 days and 364 days after birth.
Dr. Danielle Ely, co-author of the report and a health statistician at the NCHS, said 2022 was the first year there was a significant increase in the infant mortality rate in about 20 years. That the rate did not increase in 2023 shows the rise in 2022 was likely not a fluke, she said.
"So what we're seeing is that what we were hoping would be just a one-year blip is now a two-year higher rate," she told ABC News. "It is unfortunate that it did not go down again to where it was in 2021 at least or at least down from 2022. It just quite literally stayed the same, the infant mortality did."

Black infants died at a rate of 10.9 infant deaths per 1,000 live births, more than double the rate of 4.5 deaths per 1,000 live births for white women and 3.4 deaths per 1,000 live births for Asian women, per the CDC data.
Infants born to American Indian and Alaska Native women also had higher rates than white and Asian women at 9.2 deaths per 1,000 live births, according to the report.
Data also showed infants born to Hawaiian or Pacific Islander women died at a rate of 8.2 deaths per 1,000 live births, and those born to Hispanic women died at a rate of 5.0 deaths per 1,000 live births.
Why racial disparities continue to persist is "the $100 million question," Dr. Kirsten Bechtel, a pediatric emergency medicine physician at Yale New Haven Children's Hospital and an expert in infant mortality, told ABC News.
"One of things that's great about this data is that it helps us work backward. It's like the canary in the gold mine," Bechtel, who was not involved in the report, said. "Death is an outcome that everyone agrees on is a problem, but why that problem happens is oftentimes subject to vigorous discussion."
She said one reason behind the disparities could be that Black mothers have a higher rate of pre-term birth, and pre-term birth is associated with higher infant mortality.
"That has a lot to do with access to timely prenatal care," Bechtel said. "Trying to get folks access to timely care during pregnancy and timely care that is evidence-based. We also know there is some elements of structural racism that is built into some of the care these women receive."
Bechtel said the findings show that pregnant people need to be supported financially with access to medical care and by the community helping take care of a child.
"Raising a child can be very daunting, especially if you have socioeconomic challenges or you have to go to work and you can't take time off after your baby's birth," she said. "So we really need to look at policies that support pregnant people."
Harika Rayala, M.D., MSJ, is a neurology resident physician at the University of Virginia and a member of the ABC News Medical Unit.

UNC Hospitals See Spike in Walking Pneumonia Cases in Children. What You Should be Worried About.

A national spike in walking pneumonia cases is being reflected in the Triangle.
(WUNC, Abigail Celoria) -- UNC Hospitals reported 40 walking pneumonia cases in the last week of October, which includes patients tested in clinics, emergency departments, and other locations. That's compared to almost none in the same week last year.
This follows the Centers for Disease Control and Prevention's warning about the rise of mycoplasma pneumoniae infections, a bacteria that can cause walking pneumonia. These cases surfaced again in 2023 after a low following the pandemic.
Dr. Zach Willis, a pediatric infectious disease specialist at UNC Children's, says the outbreak is particularly affecting kids.
"It's much more common in children who are teenage years or, you know, down to about age 10," he said. "But, typically children under five, usually not. It's usually very rare in children who are not yet school age."
Typical symptoms of walking pneumonia include cough, fever, sore throat, difficulty breathing, and fatigue, with other symptoms appearing in children. What's unusual about the outbreak this year is its bacterial cause.
"If a three-year-old had walking pneumonia (before), I would say they probably have a viral infection," said Willis. "But more recently, if a three-year-old had walking pneumonia, I would say there's a good chance that they have mycoplasma (pneumoniae)."
Despite the spike, Willis stressed that parents don't have to worry.
"We all know that this time of year, especially if you have kids in school or in daycare, respiratory infections are common," he said. "And, this is just a different thing that has occurred this year. But, it is helpful for people to be aware, because if a child does have fever, sore throat, or cough that's persistent, then that can be made better."
According to Willis, it's also helpful for clinicians to be aware, since mycoplasma pneumoniae responds to a different antibiotic than what's usually used to treat pneumonia.
"So for mycoplasma (pneumoniae), specifically, hand washing and cough hygiene are very important," he said. "It's spread by coughing. And so those are ways to prevent getting infected. But, if it does happen, it is something that can be managed if the patient gets the right treatment."
FEMA Disaster Recovery Center Announces Closure
CHARLOTTE, N.C. (WBTV)—The Federal Emergency Management Agency (FEMA) Disaster Recovery Center (DRC) in Mecklenburg County announced on Wednesday, Nov. 13, that it will permanently close at 7 p.m. on Friday, Nov. 15.
Officials gave no reason as to why the center is closing; however, they did emphasize North Carolinians will still have many options for in-person help at the other 24 open DRC locations in the state.
“It is not necessary to go to a center to apply for FEMA assistance,” a spokesperson wrote. “The fastest way to apply is online at DisasterAssistance.gov or via the FEMA App.”
For additional DRC locations in the state, click here.

Will Hurricane Helene Impact Drop in NC Drug Overdose Deaths?

As drug experts parse the data trying to understand the factors that could contribute to a sudden drop in overdose deaths, harm reductionists in western N.C. work to stave off a possible spike in overdoses after the destruction brought by Hurricane Helene.
(NC Health News, Taylor Knopf) -- Just as substance use experts celebrated a somewhat mysterious drop in drug overdose deaths across North Carolina, Hurricane Helene blew through the western part of the state, causing death and widespread property damage. In the storm’s aftermath, many residents found themselves without homes and businesses and facing an uncertain future.
For harm reductionists like Hill Brown, the southern director of Faith in Harm Reduction, Helene’s impact raised serious concerns. Brown knew that the disruption to the local drug supply, coupled with the stress of losing housing, could lead to an uptick in overdoses in the coming months.
Over the past month, Brown, who lives in western North Carolina, has been pushing to get the overdose reversal drug, naloxone, into the hands of more people. Brown said she was surprised to find that some rural areas that had previously resisted harm reduction efforts, including naloxone distribution, have begun to embrace these life-saving tools in the wake of Helene.
“Once the [drug] supply comes back online, and people haven’t had good access to their dealers or to whatever supply they were using, there is going to be an uptick in overdoses, because we just don’t know what the supply is going to look like,” Brown said.
“If we’re talking about a crisis where lots of people are losing their housing, or their housing is becoming unlivable because of flooding, then people are going to be stressed out, and they’re going to do things that they know how to do to cope.”
This threat comes when the overdose crisis in North Carolina has shown signs of improvement — at least on paper. The latest data reported by the Centers for Disease Control and Prevention predicts about a 30 percent decrease in overdose deaths in North Carolina from May 2023 to May 2024, a statistic that will be confirmed once death certificates are finalized.
Nationally, the CDC estimates roughly a 13 percent decrease in overdose deaths for the same time period, based on provisional death data.
These numbers will likely shift because the data is incomplete right now, and North Carolina has been particularly slow in reporting its overdose death data to the federal agency, according to a note that initially topped the latest CDC report. Spokesperson Summer Tonizzo, with the N.C. Department of Health and Human Services, told NC Health News that this is an indication that North Carolina has a high number of “pending” deaths.
 Provisional data from the North Carolina Office of the Chief Medical Examiner’s Office shows suspected overdose deaths in the state dropping so far in 2024. Credit: North Carolina Office of the Chief Medical Examiner
Provisional data from the North Carolina Office of the Chief Medical Examiner’s Office shows suspected overdose deaths in the state dropping so far in 2024. Credit: North Carolina Office of the Chief Medical Examiner
“These are cases being investigated by NC’s Medical Examiner System which continues to struggle with rising caseloads and staff vacancies — both of which have negatively impacted the system’s ability to timely close pending death records,” Tonizzo wrote in an email.
Even so, North Carolina epidemiologists say, all indicators point to a significant decrease in overdose deaths. But as they dig into the data, a more complex picture emerges — one marked by uneven progress and disparities affecting marginalized communities.
Cautiously optimistic
Those ongoing pressures in the medical examiner system means it takes a long time to certify death reports that go through the state’s medical examiner’s office. North Carolina’s last complete year of finalized overdose death data is 2022.
“We’re almost at the end of 2024. It’s not fast enough,” Mary Beth Cox, an epidemiologist who tracks substance use at the North Carolina Division of Public Health told a NC Opioid and Prescription Drug Abuse Advisory Committee meeting in September.
Because there will always be some lag in the data, researchers like Cox look to some early indicators, such as emergency department visits, to track the state’s progress in addressing the overdose crisis. Since 2018, her department has been putting out monthly reports on overdose trends seen in emergency departments across the state. The latest report shows emergency department visits are down consistently in 2024 over the same period of time last year. For example, 1,055 overdose visits were reported in August 2024 while 1,518 were reported in August 2023.

Another early indicator researchers look at is 911 calls seeking help for an overdose. Nationally, first responders report that those calls are down 16 percent in October 2024 from October 2023.
But these systems don’t paint a clear enough picture, Cox said.
“If we’re seeing a decrease in [emergency department] data, does that actually mean a decrease in overdoses? We don’t know. It just means people aren’t going to the [emergency department],” she explained. “If we see an increase in [emergency department] visits, you might say, at face value, that’s a bad thing. But it could mean more people are getting connected to care.”
“Without the death data to supplement, it’s really hard to know what’s going on,” Cox said.
Her team has worked with the chief medical examiner’s office to put out an additional report every month on suspected overdose deaths. Their most recent report shows a 27 percent decrease in suspected overdose deaths in September 2024 from September 2023.
North Carolina Attorney General (now governor-elect) Josh Stein attended the meeting and applauded the group for their tireless work to address the opioid crisis. His office played a key role leading the multi-state legal challenges that resulted in $1.5 billion in opioid settlement money for North Carolina.
“We are starting to see some hopeful developments on the horizon,” Stein said in September. “Obviously, we are not naive. We know the work is not done. There is so much more to do. But it’s appropriate to see and appreciate that something is better today than it was yesterday because folks have been working really hard for that to happen.”
Cox cautioned that these decreases don’t appear to be uniform across all demographics. “This is still very provisional data, very subject to change. But we’re seeing it across multiple indicators that historically marginalized populations, particularly our Black communities, are still experiencing a slight increase.”
A recent analysis of national data by KFF (formerly the Kaiser Family Foundation) found that white people have experienced the greatest drop in rate of overdose deaths, and Black and Indigenous communities are still battling disproportionately higher rates of overdose deaths.

While the overall trend offers glimmers of hope, Cox acknowledged the sobering reality behind the numbers — nine people are dying by overdose every day in North Carolina.
“That’s a lot of people still,” Cox said. “Certainly we’re headed in the right direction, but it’s a whole lot of death.
“Every one of those deaths is preventable.”
Not the full picture
Those who work in harm reduction, like Michelle Mathis, executive director of Olive Branch Ministry, say the state’s surveillance data fails to capture the reality they see on the ground. Mathis’ ministry serves people who use drugs in the foothills/Western Piedmont area of North Carolina. Olive Branch offers multiple fixed syringe exchange sites and mobile programs.
“The trends that we see — and when I talk to other agencies as well — they’re not seeing this big downward reporting in overdoses,” she said.
She said that harm reduction workers always ask participants: Are you aware of any overdoses or have you personally experienced an overdose since the last time we saw you? Their answers are consistently recorded, but Mathis said the state health department only takes up that data once a year to include in an annual report.
“I have argued for this for as long as syringe services have been legal in the state. … We have to have some kind of monthly reporting mechanism,” she said.
Mathis said the majority of people that participate in Olive Branch’s exchange do not call 911 or go to the hospital when someone overdoses.
“Perhaps overdoses are not necessarily down, but people have access to more Narcan — because of harm reduction agencies — and so they are not as prone to being involved with EMS and the hospitals,” she said.
She added that a big reason her participants say they hesitate to call 911 during an overdose is fear of the state’s “death by distribution” law, which has been strengthened by the state legislature since it was enacted in 2019. The law allows prosecutors to charge someone with second degree murder if they sell drugs to someone who then dies of an overdose. Advocates say that the line between drug dealer and drug user is blurry, as people often buy and sell drugs from their friends and people they use with, who might not be what most would consider a “dealer,” per se.
Advocates say this law deters people from seeking help.
Brown, who has worked on advancing harm reduction efforts in Mitchell, Yancey and Buncombe counties, also said it’s hard to make sense of a reported drop in overdoses after witnessing the ever-changing illegal drug supply and people’s fear of potential death by distribution charges.
Why are overdose deaths declining?
These huge drops in overdose deaths being reported in North Carolina and around the country are puzzling to many. Substance use experts at the Street Drug Analysis Lab at the University of North Carolina say that a 15 percent to 20 percent decrease in drug overdoses would be “unprecedented.”
“To our knowledge, no public health intervention in the United States has ever achieved this benchmark,” members of the lab wrote in a recent blog post. “Something has changed. And that this is happening without central coordination is a big deal. It has major implications for the way we think about overdose prevention interventions.”
Adams Sibley, social behavioral scientist with UNC lab, co-authored the lengthy blog post, which digs into the many leading hypotheses for the mysterious drop — from increased naloxone distribution to law enforcement operations at the border to removal of barriers to addiction treatment.
Sibley also presented to the NC Opioid and Prescription Drug Abuse Advisory Committee in September and said the decrease is likely a combination of many things, including the presence of xylazine in the street drug supply and a shift from injecting substances to snorting or smoking.
Xylazine, a veterinary tranquilizer, is an additive that has been increasingly found in the illegal drug supply added to fentanyl or heroin. It can cause nasty wounds and potentially deadly skin infections at the site of injection.
“There’s a hypothesis that xylazine is one contributor to the drop in overdose deaths in a positive way,” Sibley explained. “Xylazine gives fentanyl legs, which means people may be using fentanyl less throughout the day because it’s prolonging the perceived effect of fentanyl. Xylazine also causes these skin injuries, and so it might be encouraging people to switch to smoking.”
Switching mode of drug consumption from injecting to smoking or snorting is a harm reduction measure because people use smaller amounts of drugs at a time. And smoking has surpassed injecting as the most common way people use drugs, according to the CDC. There are several reasons someone might switch to smoking, Sibley said.

Mathis said she has witnessed a shift toward smoking in participants of Olive Branch Ministry’s syringe exchange programs. She noted that the law that legalized syringe services programs does not allow for the distribution of smoking and snorting supplies.
“So we see — and we want to acknowledge — that change in mode of consumption is contributing greatly to this massive positive trend,” she said. “Yet state statute does not allow us to distribute the supplies which could really help boost this trend if we could legally do it.”
Sibley reminded the audience gathered in September that it’s important to stay humble, examine the data closely and listen to people who use drugs.
“We are not always in control of the numbers and the trends,” he said. “We know treatments are working. We know naloxone is working. But there may be reasons that overdose deaths are dropping that are out of our control.”

It's 'Easier for You' to Renew Your 2025 NCMS Membership
The immediate crisis caused by Hurricane Helene in Western North Carolina has subsided. Now, the long journey to full recovery is beginning.
Included on your 2025 invoice is a spot to Round Up When You Renew! The money raised will support your colleagues as they re-build, re-open, and start to care for patients again.
Also, we’ve made it Easier for You to renew your 2025 state, county, and NCMS managed specialty society dues … all on one convenient invoice.
Look for your 2025 Membership Dues Invoice in your inbox or renew online now — and remember “Round Up and Renew” and it’s “Easier for You.”

Hurricane Helene Disaster Response: Help for Helpers. Because You are NOT Alone!
In a disaster, it's essential that first responders and volunteers have the resources they need—when and where they need them.
If you are a first responder or volunteer experiencing stress, emotional fatigue, a mental health crisis or just need someone to talk to, you can call the Hope4NC Helpline, 1-855-587-3463. Hope4NC is free, confidential, and available 24/7.
Hope4NC is a Crisis Counseling Program which will provide immediate support and crisis counseling services for responders and volunteers providing Hurricane Helene disaster response.

HHS Releases Sexually Transmitted Infections Progress Report and Herpes Simplex Virus Addendum

The U.S. Department of Health and Human Services (HHS) released the 2021–2023 Progress Report - PDF for the Sexually Transmitted Infections National Strategic Plan for the United States: 2021–2025. The progress report provides a high-level overview of progress on select federal agency programs, policies, research, and other activities during fiscal years 2021–2023.
The progress report features an at-a-glance table of the status of seven core indicators and seven disparities indicators, which were identified in the national plan as a quantitative approach to measuring progress on STI prevention and care in the United States. The most recently available data reveal that seven of the indicators have met or are moving toward annual targets and that seven have not met or are moving away from annual targets. Of this latter group, six indicators relate to syphilis, which is the focus of the National Syphilis and Congenital Syphilis Syndemic Federal Task Force led by HHS Assistant Secretary for Health, Admiral Rachel Levine, M.D.
“These data serve as a call to action for continued collaboration in our national response to STIs,” said Admiral Levine.“ Through education, awareness, and increased access to care, we can improve outcomes of syphilis, and other STIs, and safeguard the health of communities across our nation.”
Building on federal efforts to meaningfully prevent and control STIs in the United States, the Herpes Simplex Virus (HSV) Addendum to STI National Strategic Plan sets a unified national response to HSV. HSV is a lifelong condition that spreads primarily from skin-to-skin contact and is one of the most common STIs in the United States. Most people with HSV are asymptomatic and undiagnosed. For those who are symptomatic, HSV can cause recurring outbreaks of painful sores on the mouth or genital areas, and the stigma associated with HSV can significantly impact quality of life.
HSV was not initially included in the national strategy, which focused on chlamydia, gonorrhea, syphilis, and human papillomavirus. This is because the plan originally focused on STIs in the United States for which there are federally funded control programs. Additionally, HSV is not a nationally notifiable condition and there is no existing national surveillance system for HSV or neonatal herpes to measure progress. Likewise, diagnosing genital herpes can be challenging, since many people do not have symptoms.
“HSV is a critical priority for us. Future iterations of the STI Plan will incorporate HSV within its purview. HHS will work with communities who are underserved and disproportionately affected to prevent HSV and improve access to care, while also advancing health equity and reducing stigma,” said Kaye Hayes, Deputy Assistant Secretary for Infectious Disease and the Director of the Office of Infectious Disease and HIV/AIDS Policy.
The development of the HSV Addendum was guided by principles focused on integrating the latest science; prioritizing federal actions; leveraging existing infrastructure, capacity, and resources; and coordinating action between national, state, territorial, tribal, and local community organizations and members. [source]
Read the 2021–2023 STI Progress Report - PDF
Read the HSV Addendum - PDF
Read the STI Federal Implementation Plan - PDF
Read the STI National Strategic Plan - PDF
Join the American Indian Respiratory Health Initiative Fireside Chat and Tele-town Hall on November 14
The North Carolina Department of Health and Human Services, in collaboration with the North Carolina Commission of Indian Affairs, will host a live fireside chat and tele-town hall on Thursday, November 14, from 6 to 7 p.m., to discuss the updated flu and COVID-19 vaccines and other steps to protect tribal communities against severe respiratory illness, hospitalization and long-term respiratory health complications. Panelists will also discuss ways people can find nearby health care providers and access care, as well as how to access free or low-cost vaccines.
The town hall is part of an ongoing initiative to raise awareness of respiratory illnesses, promote vaccination and improve the overall health of American Indian communities throughout North Carolina. The initiative is guided by a newly formed American Indian Respiratory Health Advisory Group, composed of leaders and health care providers throughout North Carolina’s tribal communities.
Event participants include:
- Greg Bryant, Health Committee Chairperson, North Carolina Commission of Indian Affairs
- Katie Lowry, M.D., MPH, Pediatrician, Robeson Pediatrics
- Aiyana Lynch, Development & Marketing Director, The CARE Clinic
The fireside chat will stream live from the NCDHHS Facebook and YouTube accounts, where viewers can submit questions. The event also includes a tele-town hall, which invites people by phone to listen in and submit questions. People can also dial into the event by calling 855-756-7520 Ext.114212#.
The American Indian community is among those most severely impacted by respiratory viruses — double that of white, non-Hispanic individuals. Seasonal vaccines are the best way to prevent people ages 6 months and older from experiencing severe cases of flu and COVID-19, especially for those who are at a higher risk of complications from the viruses. This includes people who are under 5 and those 65 and older, pregnant and/or living with chronic medical conditions. Updated vaccines are needed even if individuals have received vaccinations in the past. The updated vaccines were developed to protect against current virus strains.
In addition to flu and COVID-19 vaccines, RSV vaccines are now available for older adults and pregnant women. Some babies and children under 2 may also need to receive an immunization to help build protection against RSV.
Testing and treatment are available to catch virus cases early and help prevent severe illness. Reach out to a health care provider as soon as symptoms begin to test for the flu, COVID-19 or RSV and see if treatment is needed.
Visit MySpot.nc.gov for information, guidance and resources on seasonal vaccines and how they support respiratory health. [source]

Diabetes Performance Improvement in Primary Care
Diabetes Performance Improvement in Primary Care - Enduring
Online Self-Paced Learning
Free for the first 100 to register!
Complete at your own pace
This educational activity aims to inform the learner about the status of diabetes and chronic kidney disease in primary care. This activity will explore barriers and facilitators to promote patient engagement in treatment. This activity will focus on performance improvement methods and activities which promote health among patients with diabetes.
Objectives
- Describe barriers and strategies for clinical care teams in the screening, diagnosis, and treatment of patients with diabetes and chronic kidney disease (CKD).
- Utilize new methods to identify how diabetes and CKD disproportionately affect racial and ethnic minorities in clinical workflows.
- Explain processes for screening, diagnosis, and raising awareness about diabetes and its connection to chronic kidney disease (CKD).
For more information and to register, click here.

North Carolina Hospitals See Surge in Pediatric Pneumonia Cases
‘A-typical pneumonia’ is landing more children in Triangle-area hospitals for treatment.
Mycoplasma pneumonia, often referred to as ‘a-typical pneumonia’ is landing more children in Triangle-area hospitals for treatment.
It’s the same kind of bacteria that causes walking pneumonia.
Dr. Zachary Willis, UNC Children’s pediatric infectious disease specialist, explained the case volume the area is currently seeing is “a bit unusual.”
“Commonly, we would see it in older children and teenagers but recently we’re seeing it more in younger children which is something of a surprise,” Willis said. “Children as young as 2 years old we’re seeing with us.”
Willis explained that most who get sick with this type of pneumonia can recover on their own.
“There is no vaccine for this specific type of infection but there are antibiotics that are effective,” Willis said.
UNC Hospitals reports 40 positive cases of mycoplasma pneumonia were reported during the last week of October 2024. During that same period last year, zero cases were detected.
Read the full article here.

Join the Community Alternatives Program Fall Provider Webinar
NC Medicaid Long Term Services and Supports (LTSS) will host a Fall Provider webinar on Community Alternatives Program (CAP) services Wednesday, November 20, 2024, from 9 a.m. to 12 p.m.
Providers who support Community Alternatives Program for Children (CAP/C) and Community Alternatives Program for Disabled Adults (CAP/DA) Medicaid beneficiaries enrolled in NC Medicaid Direct will receive updates and have an opportunity to ask questions.
To register, visit the NCLIFTSS (Acentra) web page.
The webinar will cover:
- Hurricane Helene disaster recovery efforts
- CAP Population Census and Health Disparity Report
- Proposed data to display on the CAP Dashboard
- CAP/DA waitlist management process
- CAP/DA Renewal Waiver update
- CAP/C Utilization of attendant nursing care (ANC), pediatric nurse aide (PNA) and In-home aide (IHA) services in combination with other Medicaid and waiver services
- CAP Measurements of Continuous Quality Improvement Strategies
Contact: NCLIFTSS (Acentra) or 833-522-5429

Register Now! PANS and Related Inflammatory Brain Disorders – Advances in Immunopsychiatry
Join Us for On-Demand CME –Free to North Carolina Physicians
PANS and Related Inflammatory Brain Disorders: Advances in Immunopsychiatry features nationally and internationally renowned experts skilled in diagnostic and therapeutic approaches who will present a diverse range of emerging clinical and research challenges, insights, and advances in the field of inflammatory brain disorders.
Download the pdf here.
NCDHHS: Notification Required for Change of Ownership
Enrolled providers must notify the Department at least 30 days prior to the effective date of a change of ownership.
Consistent with state and federal law, NCDHHS requires notification of any change of ownership (CHOW) for providers enrolled as a NC Medicaid provider. The enrolled provider must notify the Department at least 30 days prior to the effective date of any CHOW.
Providers will need to complete the Provider Change of Ownership Disclosure Form. The form is located on the NCTracks Providers webpage under Quick Links.
Once the form is downloaded, the Provider will need to:
- Complete all applicable fields within the CHOW form
- Email the form and any supporting documentation to [email protected]
In addition to submitting the Disclosure Form, both the former and new owner must make changes to the provider’s NCTracks enrollment record. For information regarding the enrollment, termination or modification of the NCTracks Provider Enrollment record due to a CHOW, review the Change of Ownership (CHOW) FAQs and follow the instructions as applicable to the intended structure of the NCTracks enrollment record under the new owner.
Questions? Contact: NCTracks Call Center: 800-688-6696

Joy, Giving, and Community Spirit: 20th Annual Cheers! for Brenner Children's Hospital
The 20th Annual Cheers! for Brenner Children's Hospital will take place Friday, November 15, at the Millennium Center in downtown Winston-Salem.
Organizers are promising an extraordinary evening filled with joy, giving and community spirit. The event is presented by Simply Southern, which has committed to match all funds raised, up to $150,000, amplifying the impact of each dollar donated.
Atrium Health Levine Children’s Brenner Children's Hospital in Winston-Salem, a full-service children’s hospital serving western North Carolina, is the Triad region’s only children’s hospital, pediatric emergency department, Level I children’s surgery center and Level I pediatric trauma center, a distinction it has held since 2011 when it became the first in the state.
Since its inception in 2005, Cheers! has raised over $3 million, with funds helping Brenner Children's Hospital deliver critical services, advance research and ensure that every patient receives exceptional care. Over the years, this beloved event has become a heartfelt tradition, bringing together generous individuals, former patients, families and friends, all united in support of Brenner Children’s Hospital’s mission.
To celebrate its 20th anniversary, Cheers! will feature an array of activities, including a seated dinner, specialty cocktails and both live and silent auctions. The evening will conclude with an energetic late-night silent disco, providing a unique experience to cap off a memorable night.
“As we celebrate 20 years of Cheers! for Brenner Children's Hospital, we’re reminded of the incredible impact our community’s support has had," said Lisa Marshall, chief philanthropy officer and vice president at Atrium Health Wake Forest Baptist. "This longstanding generosity has allowed us to expand our reach and elevate our services, ensuring that we can continue making a profound difference in the lives of countless children and families. Together, we’re building a legacy of hope that grows stronger every year."
More information about the 20th annual Cheers! for Brenner Children's Hospital, including ticket sales and sponsorship opportunities, can be found at BrennerChildrens.org/Cheers.
“We encourage our community to join us on Friday, Nov. 15 for an unforgettable evening of celebration, unity, and philanthropy as we work together to make a difference in the lives of children in need,” Marshall said. [source]
Two NC HBCUs Partner with Duke to Increase Black Student Representation in Medicine

(WUNC, Brianna Atkinson) -- Two of the state's private Historically Black Colleges and Universities (HBCUs) are partnering with Duke University to increase representation in the medical field. Students from Bennett College, a women's-only institution in Greensboro, and Saint Augustine's University in Raleigh will participate in a 15-month intensive program to study otolaryngology (ear, nose, and throat) and communication sciences.
According to the American Medical Association, otolaryngology has especially low numbers of women and Black people compared to other medical specialties. Women make up about 2.5% of the field and Black people just 1.1%.
Dr. Dennis Frank-Ito is leading the program at Duke University. He said in his experience, many Black students aren't aware of otolaryngology and communication sciences until they are already deep into their undergraduate studies.
"Which might be too late for them to start taking the right classes in preparation for this," Frank-Ito said. "There's a critical need (because) we know that for Black and African American patients, if there is a concordance between the patient and the provider that often leads to better health outcomes."
According to a 2023 study from the National Institutes of Health (NIH), there are "significant healthcare disparities in care and treatment outcomes" for underrepresented groups in otolaryngology. The study found that Black patients have higher instances of HPV and oropharyngeal cancer, as well as a lower survival rate compared to white patients.
Frank-Ito hopes the program at Duke, which will run for at least five years, will help more Black students gain interest in the field.
"We are hoping that in the next 10 years we can see that through this program we have more Black professionals in our field," Frank-Ito said. "And when we look at health outcomes for Black and other minority populations – especially in the Triangle area – there's an improvement in how patients feel when they see specialists in our field. That's the legacy we plan to leave behind."
In each cycle, there will be three rising juniors from Bennett College and Saint Augustine's University. At least one student will come from each university.
The cohort will stay on Duke University's campus for the summer, where they will participate in clinical trainings and professional development. This can range from classes about how COVID-19 affects the sense of smell to how to gather data from online libraries. The program is being funded through an R25 grant from the NIH.
After the summer sessions, students will work with Duke faculty remotely for the remainder of the 15-month cycle. Frank-Ito said all students that apply to the program will have access to these virtual trainings and materials.
"So even though they were not selected, they still have enough information from this training program to have the right exposure, whether or not to pursue a career in our field," Frank-Ito said. "Our lasting impact is to increase representation in our field. We want to ensure that through this program, we are going to be able to pave the way for more Black professionals in otolaryngology and communication sciences."
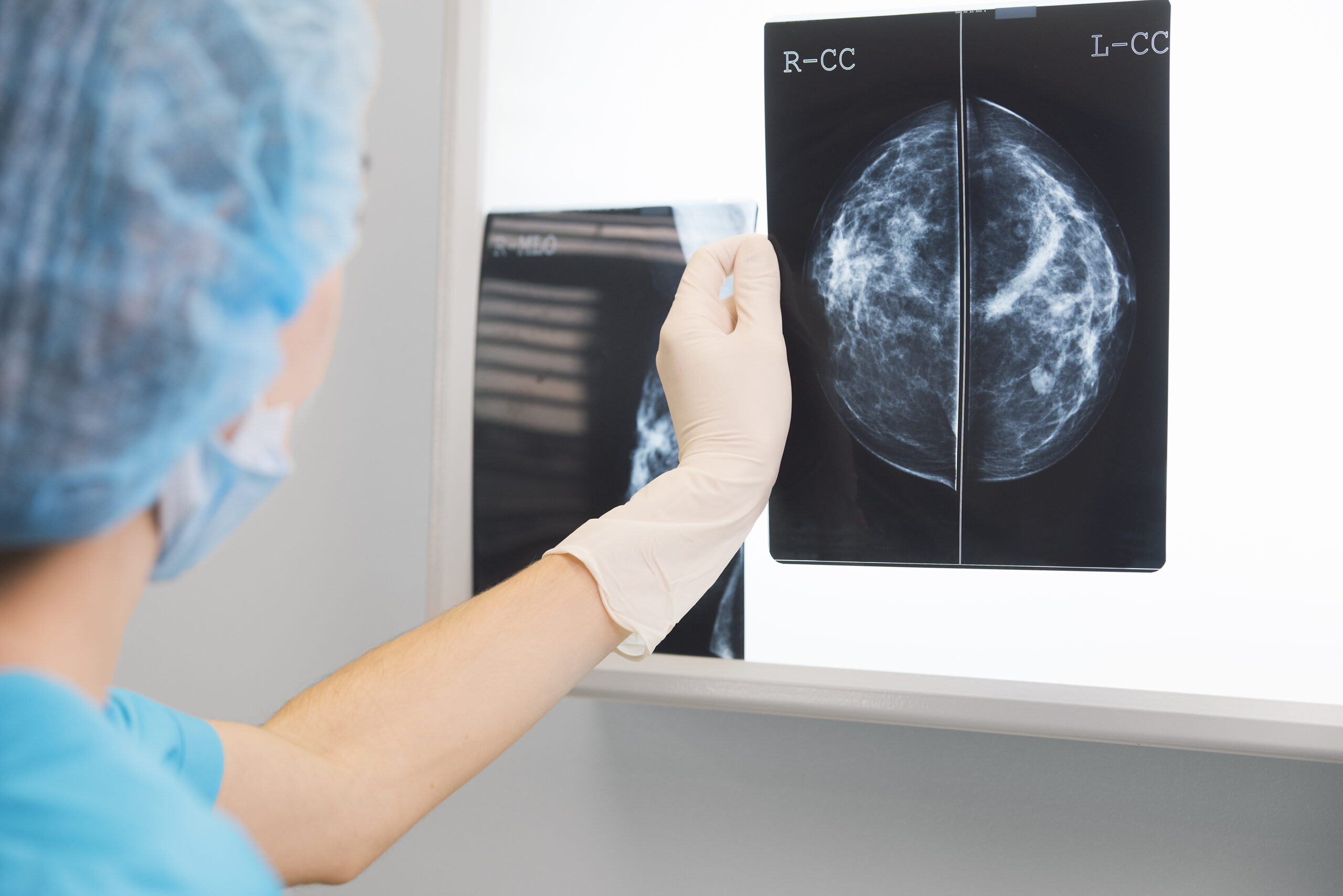
Enhanced Breast Cancer Screening for Women with Dense Breast Tissue
AdventHealth Hendersonville is excited to announce the availability of contrast-enhanced mammography (CEM) for patients in Western North Carolina, particularly benefiting women with dense breast tissue. The CEM is available through AdventHealth Imaging Hendersonville’s Hologic 3Dimensions® mammography system.
Recent research has shown that standard mammography can be 30% to 40% less sensitive in women with dense breast tissue. Studies prove that contrast-enhanced mammography is especially effective on dense breasts because it is unaffected by background breast tissue, making it an easier and more effective exam.
In the U.S., mammograms are recommended yearly or bi-yearly for people aged 40 to 74.
According to the National Cancer Institute, nearly half of women 40 and older who get mammograms have dense breasts. For women with dense breast tissue, or women with a high risk of cancer, contrast-enhanced mammography offers the ability to find cancer earlier.
With contrast-enhanced mammography before the patient has the imaging scans, they are given contrast dye through an IV. This dye shows up in the scans and allows for cancer to be recognized at the earliest possible stages. Contrast-enhanced mammography is also proven to reduce the number of biopsies on women who might not have cancer.
AdventHealth encourages women who are interested in this new cancer screening and diagnostic tool to talk with their doctor to find out if contrast-enhanced mammography is the right option for them. Patients may qualify for CEM cancer screening if they have dense breast tissue, intermediate risk of cancer, or are at high risk but do not qualify for MRI or would prefer CEM.
Extended Imaging Hours:
To make it easier for patients to receive the imaging services they need, AdventHealth now offers Extended Imaging Hours at our hospital in Hendersonville. Patients can call 828-681-2180 to schedule imaging appointments until 8 pm on Tuesdays and Thursdays.
AdventHealth Hendersonville is committed to providing comprehensive cancer care you can count on. With this new state-of-the-art cancer screening and diagnostic tool, women in WNC can have peace-of-mind knowing that AdventHealth is making it easier and more convenient to catch their cancer early.
To learn more or schedule an appointment, visit AdventHealthWNC.com or call 828-681-2180. [source]
Register Now! Psychiatric Presentations with a Neuroimmune Basis ECHO
Neuroimmune Foundation has partnered with Project ECHO® – an internationally recognized platform with over one million learners in 45+ countries focused on over 1000 medical conditions, to offer weekly didactics and case-based learning to physicians worldwide.


Download the pdf document here.
Register here.

🎉It's New Member Monday!🎉
Join us in welcoming these new members to the North Carolina Medical Society!
- Ian Adam, MD
- Catherine M. Alexander, MD
- Yonghee K. Cho, MD
- Nicola S. Corbett, MD
- Jakub M. Dmochowski, MD
- Michael B. Geary, MD
- John W. Henderson, II, DO
- Andrew S. Hodge, DO
- Kyle C. Lambert, PA-C
- David M. Macknet, MD
- Lauren S. Mokris, MD
- Jessica R. Swavely, DO
- Trishna Chand Thakur, MD
- Paul R. Weaver, DO
We are thrilled to have you!
Not a member but would like to be? Joining is simple. Visit our membership center here.
A Message from the U.S. Surgeon General’s Office: Protecting the Wellbeing of the Clinical Workforce
A Message from the U.S. Surgeon General’s Office
“We know that better is not only possible but is vital before any more lives are lost among us or impacted further by the stigma that surrounds mental health. Health workers, in particular, now more than ever, deserve the care, treatment, and support they need, whenever they need it, and without any shame or fear of losing their health professional licenses, jobs, even careers.”
Jeane Garcia Davis, MSN/MPH, RN
Deputy Director for Science and Policy
U.S. Surgeon General’s Office

Jeane Garcia Davis, Deputy Director for Science and Policy at the U.S. Surgeon General’s Office, shares a video message with North Carolina physicians, PAs, trainees, residents, and students. In her message, she underscores national efforts to protect the wellbeing of the clinical workforce, highlighting landmark policies and investments aimed at transforming structures, systems, and workplace cultures. She emphasizes that the wellbeing of our nations and state’s health workers is just as vital as that of the patients they care for.

Key Stretch of Blue Ridge Parkway Reopens After Hurricane Helene Damage
Hurricane Helene carved a path of devastation across the southeastern United States in September and left areas like the Blue Ridge Mountains around Asheville, North Carolina in complete destruction. Now, less than two months later, an important part of the scenic Blue Ridge Parkway is once again open to drivers.
On November 6, the Blue Ridge Parkway announced that it reopened an 11-mile stretch of the famous road near Asheville. The newly reopened portion reaches from milepost 382.5 at U.S. 70 near the Folk Art Center to milepost 393.6 at NC Route 191 near the North Carolina Arboretum and the French Broad Overlook at milepost 393.8.
Continue reading here.

NCMS Recognizes NCMS Disaster Relief Fund Contributors
A heartfelt THANK YOU to these individuals and organizations for their contribution to the NCMS Disaster Relief Fund. Your generous donation is far more than just a financial contribution; it’s a lifeline for the many affected by Hurricane Helene, and vital in providing support to healthcare professionals and communities impacted by this disaster.
We invite you to spread the word about the NCMS Disaster Relief Fund and stay engaged with us as we work together to help restore our Western North Carolina neighbors.
We are grateful to have you in our community!
- American Medical Association Foundation
- Atlantic Internal Medicine
- Amar M. Amaresh, MD
- Edwin C. Bartlett, Sr., MD
- Deanna M. Boyette, MD
- Edwin K. Burkett, MD
- Cobb County (GA) Medical Society
- John A. Fagg, MD
- Barbara Hodde
- Martha G. Peck, MD
- Gary Price, MD
- Eugene E. Wright, Jr., MD
- Kathy F. Wright
- Curi
- Anonymous
- Christopher T. Grubb, MD
- Lyndon K. Jordan, III, MD, FACR
- Katie Lowry, MD, MPH
- Laura J. Luckadoo, MD
- Robeson Pediatrics
- Kirby Sheridan
- Catherine L. Sotir, MD
- Vinod C. Vallabh, MD
- Ian D. Archibald, MD
- Preecha Bhotiwihok, MD, MPH
- John W. Black, MD
- Anonymous
- Gay M. Bowman
- Georgi N. Brockway, MD
- Michael T. Brohawn
- Anonymous
- Carolina Complete Health Network
- Sharon M. Foster, MD, FAAP
- Donna C. Graves, MD
- M. Mark Hester, MD
- Suneya G. Hogarty, DO
- Marius J. Ilario, MD
- Linda W. Lawrence, MD
- Douglas S. McFarlane, MD
- Mark B. Moeller, MD
- Anonymous
- Raleigh Orthopaedic Clinic, PA
- Timothy J. Reeder, MD, MPH, FACEP
- Alan J. Rosenbaum, MD
- Anonymous
- Marshall Z. Schwartz, MD
- Douglas D. Sheets, MD, FACOG
- W. Alan Skipper, CAE
- Jennifer K. Stoddard, MD
- STUSQU, PLLC
- Lisa W. H. Thompson, MD
- Cheryl L. Walker-McGill, MD, MBA
- Craig E. Webb, MHS, PA-C
- Johnathan D. Williams, MD
- Anonymous
- Idil Aktan, MD
- R. D. Almkuist, II, MD
- American Board of Pediatrics Inc
- Caroline D. Ames, MD, FACS
- James H. Antoszyk, MD
- Joy Avery
- Timothy M. Beittel, MD
- Anonymous
- Anonymous
- Cedar Mount Behavioral Health, PA
- Center For Pain Management, PLLC
- Melissa M. Coale, MD
- Anonymous
- Kim D. Dansie, MD
- Jackie M. Davis-Jones
- Jessica F. Doerrler, PA
- Patricia Duncan
- Peter A. Eweje, MD
- Mark W. Featherston, MD
- Anonymous
- Joanne M. Fruth, MD
- Lisa M. Gangarosa, MD
- Highland Medical Associates
- Anonymous
- Joseph P. Hunstad, MD, FACS
- Kitsie Jones
- Christopher P. Jordan, MD
- Kerry Kendall
- Eugenie M. Komives, MD, FAAFP
- Ted R. Kunstling, MD, FCCP
- Andrew S. Lamb, MD
- Keith LaScalea, MD
- Anonymous
- Elizabeth G. Livingston, MD
- Anonymous
- Laura L. Martinez, MD
- Darlyne Menscer, MD
- Ashley Newton
- J. Thomas Newton, MD
- Carolyn O'Conor, MD
- Michael K. Patrick, MD
- Patricia Petrick, MD
- Emily Rayes-Prince, MD
- Anonymous
- Corianne D. Rogers, MD
- Nimesh B. Shah, MD
- Kristen M. Shipherd
- Maria J. Small, MD
- Anonymous
- Michol Stanzione, DO
- Steele Creek Dermatology
- Al Steren, MD and Diane Snyder Steren, MD
- Martha Strange, MD
- Thomas M. Swantkowski, MD, AGAF, FACG
- Marian L. Swinker, MD, MPH
- Christopher L. Tebbit, MD
- Monecia Thomas, PhD
- Dimitri G. Trembath, MD
- Michael J. Utecht, MD, FACEP
- Lynnea Villanova, MD
- Bonnie E. Wagner, PA-C
- Rebecca Y. Weinshilboum, DO
- Carl J. Westcott, MD
- Thomas R. White, MD
- Anonymous
- Women's HealthCare Consultant PC
- Nagarjuna Yerra, MD
- Michael Bartiss, MD / Family Eye Care of the Carolinas
- David Boone, MD
- Carolina Complete Health
- Karl Chiang, MD
- John Chretien, MD
- Anonymous
- Kelly Fedoriw, MD
- Carolyn Ferree, MD
- Alison Gardner, MD
- John Goldfield, MHS, PA-C
- Akilah Grimes, MD
- Sandra Jackson / Eastern Pediatrics
- Matthew Katz, MS / MCK Health Strategies
- Melissa Kenny
- Donna McGee, MD
- Larry Napolitano, Jr., MD
- Michael P. Reddy-Miller, MD
- Anonymous
- Andrew Pasternak, MD
- Antonio Ramirez, MD
- Beth Remhof
- Jennifer Root, MD
- Richard Savage, MD
- Anonymous
- Soma Sengupta, MD
- Nimesh Shah / Noble Hospitality Investment
- Amanda Trimpey, MD, MPH, FACOEM
- Yunxiang Zhu, MD
*Please note: List reflects donations received through Tuesday, November 5.

‘Not Medically Necessary’: Inside the Company Helping America’s Biggest Health Insurers Deny Coverage for Care

Who is Really Making the Decisions?
This story was originally published by ProPublica. It co-published with The Capitol Forum.
ProPublica is a nonprofit newsroom that investigates abuses of power. Sign up to receive its biggest stories as soon as they’re published.
Every day, patients across America crack open envelopes with bad news. Yet another health insurer has decided not to pay for a treatment that their doctor has recommended. Sometimes it’s a no for an MRI for a high school wrestler with a strained back. Sometimes for a cancer procedure that will help a grandmother with a throat tumor. Sometimes for a heart scan for a truck driver feeling short of breath.
But the insurance companies don’t always make these decisions. Instead, they often outsource medical reviews to a largely hidden industry that makes money by turning down doctors’ requests for payments, known as prior authorizations. Call it the denials for dollars business.
The biggest player is a company called EviCore by Evernorth, which is hired by major American insurance companies and provides coverage to 100 million consumers — about 1 in 3 insured people. It is owned by the insurance giant Cigna.
A ProPublica and Capitol Forum investigation found that EviCore uses an algorithm backed by artificial intelligence, which some insiders call “the dial,” that it can adjust to lead to higher denials. Some contracts ensure the company makes more money the more it cuts health spending. And it issues medical guidelines that doctors have said delay and deny care for patients.
EviCore and companies like it approve prior authorizations “based on the decision that is more profitable for them,” said Barbara McAneny, a former president of the American Medical Association and a practicing oncologist. “They love to deny things.”
EviCore says it scrutinizes requests to make sure that procedures recommended by doctors are safe, necessary and cost-effective. “We are improving the quality of health care, the safety of health care and, by very happy coincidence, we’re also decreasing a significant amount of unnecessary cost,” an EviCore medical officer explains in a video produced by the company.
But EviCore’s cost-cutting is far from coincidental, according to the investigation.
EviCore markets itself to insurance companies by promising a 3-to-1 return on investment — that is, for every $1 spent on EviCore, the insurer would pay out $3 less on medical care and other costs. EviCore salespeople have boasted of a 15% increase in denials, according to the investigation, which is based on internal documents, corporate data and dozens of interviews with former employees, doctors, industry experts, health care regulators and insurance executives. Almost everybody interviewed spoke on condition of anonymity because they continue to work in the industry.
An analysis of the company’s own data shows that, since 2021, EviCore turned down prior authorization requests, in full or in part, almost 20% of the time in Arkansas, which requires the publication of denial rates. By comparison, the equivalent figure for federal Medicare Advantage plans was about 7% in 2022.
EviCore has several ways to cut costs for insurers. Chief among them is the dial, the proprietary algorithm that’s the first stop in evaluating a prior authorization. Based on data entered by a doctor’s office, it can automatically approve a request.
The algorithm cannot say no, however. If it finds problems, it sends the request for review to a team of in-house nurses and doctors who consult company medical guidelines. Only doctors can issue a final denial.
This is where tweaking the dial comes in. EviCore can adjust the algorithm to increase the number of requests sent for review, according to five former employees. The more reviews, the higher the chance of denials.
Here’s how it works, the former employees said: The algorithm reviews a request and gives it a score. For example, it may judge one request to have a 75% chance of approval, while another to have a 95% chance. If EviCore wants more denials, it can send on for review anything that scores lower than a 95%. If it wants fewer, it can set the threshold for reviews at scores lower than 75%.
“We could control that,” said one former EviCore executive involved in technology issues. “That’s the game we would play.”
Over the years, medical groups have repeatedly complained that EviCore’s guidelines were outdated and rigid, resulting in inappropriate denials or delays in care. Frustration with the rules has led some doctors to refer to the company as EvilCore. There is even a parody account on X.
The guidelines are also used as a tool to cut costs, the investigation found. Company executives “would say, ‘Keep a closer eye on the guidelines for reviews for a particular company because we’re not showing savings,’” said a former EviCore employee involved in the radiation oncology program.
EviCore says that it develops its guidelines with the input of peer-reviewed medical studies and professional societies, and that they are routinely updated to stay current with the latest evidence-backed practices. It said its decisions are based solely on the guidelines and are not interpreted differently for different clients.
EviCore is not alone in engaging in the denials-for-dollars business. The second-biggest player is Carelon Medical Benefits Management, a subsidiary of Elevance Health, the health insurer formerly known as Anthem. It has been accused in court of wrongfully denying legitimate requests for coverage. The company has denied all charges. Several smaller companies do the same kind of work.
There is no question that prior authorizations play an important role in modern medicine. They serve to guard against doctors who recommend unnecessary and even potentially harmful treatments. They also protect insurers from fraudulent physicians who overbill for services.
In a response to questions, a Cigna spokesperson provided a statement on behalf of EviCore. “Simply put, EviCore uses the latest evidence-based medicine to ensure that patients receive the care they need and avoid the services they do not,” it said.
The statement acknowledged that EviCore used algorithms for some clinical programs, but “ONLY to accelerate approval of appropriate care and reduce the administrative burden on providers.”
The statement noted that doctors have the ability to appeal prior authorization denials, and that the company routinely monitors the outcomes “as part of our continuous quality improvement to ensure accurate and timely medical necessity decision-making.”
Prior authorization reviews provided by EviCore save money for the entire health insurance system, the statement said. “The natural product of improved care quality and reduced waste is savings for our clients, lower out-of-pocket costs for patients, and fewer health care premium increases for Americans.”
Turning the dial
In the fall of 2021, when the air grew crisp and the leaves reddened in central Ohio, Little John Cupp began feeling short of breath. He gasped while pushing a shopping cart. His feet and ankles swelled. He could only sleep while sitting up.
An echocardiogram revealed that his heart was having trouble pumping blood. Cupp’s doctor suggested more testing, including the insertion of a catheter to examine whether his arteries were blocked.
A few days after the doctor made the request, Cupp received a letter from his insurance company, UnitedHealthcare. The procedure, it said, was “not medically necessary.”
One sentence in 8-point type revealed that the insurer had outsourced the decision to EviCore.
Cupp’s doctor put him on medications to reduce swelling and high blood pressure and tried a second time to win approval for a left heart catheter examination. EviCore turned it down again. He revealed his disappointment in shorthand in Cupp’s medical records: “ideally he needs LHC (denied twice by insurance).”
Cupp was 5-foot-7 and 282 pounds, with a wedding ring the size of a quarter. He had a white beard, his face wide and warm. He wore blue jean overalls and scuffed leather work boots. He had spent most of his life as a welder, working at metal fabrication shops in and around his hometown of Circleville, Ohio, population 14,063. He was 61, nearly the same age as his father when he died from a massive heart attack. Cupp was a stoic, his daughter Chris said, but the denial worried him.
“Well, I have to call the doctor and see what we’re going to do,” he told her after the second rejection.
The doctor decided to give up on getting an approval for the catheter exam. In challenging EviCore, he was fighting not just a company but an industry.
EviCore is the product of a massive, decadeslong push by insurance companies to control health care costs. They point to studies that show 20% to 45% of some medical treatments are wasteful or ineffective. To decrease such spending, insurers began requiring doctors to seek permission for medical care before agreeing to pay for it — a process known as “utilization review.” As treatments became more complex, the reviews proved costly in themselves.
Created from a 2014 merger of two smaller companies, EviCore offered a solution: It allowed insurers to outsource prior authorization decisions for the most specialized and expensive procedures. EviCore today issues recommendations for imaging, oncology, cardiology, gastroenterology, sleep problems and many other fields.
It works with more than 100 insurers across the country, including industry titans such as UnitedHealthcare, Aetna and Blue Cross Blue Shield and some Medicare and Medicaid contractors. Cigna took over the company in 2018, but EviCore maintains its independence by blocking insurers from prying into one another’s proprietary data.
In responses to inquiries, the large insurance companies said they hired EviCore as a way to make sure that customers received safe and necessary medical treatments, while holding down costs for inappropriate care.
EviCore built its business by relying on different types of contracts. In one, a health insurance company pays EviCore a flat rate to review coverage requests.
Another type is more lucrative, providing an incentive for EviCore to cut costs, former employees said. Known as risk contracts, EviCore takes on the responsibility for paying claims. As an example, say an insurer spends $10 million a year on MRIs. If EviCore keeps costs below that figure, it pockets the difference. In some cases, it splits the savings with the insurance company.
“Where you really made your money was on a risk model,” a former EviCore executive said. “Their margins were exponentially higher.”
EviCore teams involved in developing the algorithms and contracting with clients “operate separately” from reviewers “to prevent any potential conflicts of interest,” according to the statement from Cigna’s spokesperson.
Insurers do not make explicit demands for more denials, a former EviCore sales executive said, Instead, they asked about “controlling the spend” — the amount of money paid out on certain procedures, he said. Nor would EviCore always use the word “denials” — they employed circumlocutions like “inappropriate determinations.”
Aetna and Cigna are two of the companies that have requested “high touch” plans — those that would send more cases to clinical review and thus generate more denials, according to the former employee involved in data issues.
Aetna did not directly respond to whether it used “high touch” plans. “Although we never automate medical necessity denials, we automate and provide real-time approval of some services to ease administrative burden and allow providers to focus on patient care,” the insurer said in a statement. Cigna did not respond to questions about its use of such plans.
“When you have human eyes on something, you can pick up where there might be a gray area where the algorithm might not pick up,” a former EviCore account executive said. “That is how you would increase the denial rate.”
EviCore can also adjust the algorithm to achieve its internal goals, without the knowledge of clients, former employees said. This happened when EviCore was not generating enough savings to demonstrate its value to insurers, several former employees told ProPublica.
“The pressure from our business leaders was to make sure that we were able to provide evidence of a strong enough impact to justify the contracts with clients,” said the former employee involved with technology.
The system also runs in reverse. When doctors or employer health plans complain about high rejection rates, insurance companies can ask EviCore to back off. The company simply adjusts its algorithm to approve more prior authorization requests.
Dave Jones, a former California insurance commissioner and now director of the climate risk initiative at the University of California, Berkeley School of Law, said arbitrarily increasing or decreasing manual reviews didn’t appear to violate any standards. Still, he questioned whether a payment structure or contract for EviCore based on reducing claims payments or authorizations would result in objective and thorough evaluations of prior authorization requests, as required by law.
“That to me is troubling,” Jones said. “It suggests that the claim settlement procedure is not objective, right?” He added, “It calls into question everything that’s occurring.”
Other industry experts found the manipulation of denial rates upsetting.
“The fact that these big companies focused on profits and can play all these games is quite disturbing to me,” said Martin Lustick, a former insurance executive and the author of a book on industry practices. “They know the more reviews they do, the more denials they get.”
Disputed guidelines
On March 2, 2022, Cupp and his daughter entered the Adena Regional Medical Center, a gray and glass building surrounded by central Ohio’s low rolling hills.
It had been almost three months since EviCore first turned down coverage for the catheterization. Changing tack, Cupp’s doctor ordered a new exam, which EviCore approved, called a nuclear stress test. It shows how well blood flows through your heart.
A heart catheterization generally costs around $3,500 when done in network, according to Fair Health, a nonprofit that tracks health care prices. A nuclear stress test runs about $315.
Afterward, Cupp greeted Chris in the waiting room. He told her he felt fine. They went for lunch at a favorite hamburger spot. At the time, they did not know the results of the stress test, which showed that his heart was pumping even less blood than indicated by his echocardiogram.
At each step of the way, EviCore had steered Cupp’s medical treatment by denying or approving his doctor’s coverage requests based on its own internal guidelines.
Those guidelines have long been the subject of complaints from doctors. Over the past five years, organizations ranging from the American College of Cardiology to the Society for Vascular Surgery to ASTRO, the American Society for Radiation Oncology, have written to EviCore or regulators that the guidelines are flawed and can interfere with delivering the right care for patients. Benjamin Durkee, a doctor who chairs ASTRO’s payor relations committee, said EviCore had generally made “a good faith” effort to respond to the society’s concerns. But, he noted, the company continues to consistently deny a radiation treatment called proton beam therapy for some pelvic tumors that is more costly but supported by ASTRO’s recommendations.

A 2023 academic study examined the criteria EviCore used to approve payment for imaging of the lower spine in cases of extreme pain. It found the guidelines deficient. Two of five medical experts who reviewed the guidelines even recommended not using them.
A 2018 audit by the Centers for Medicare and Medicaid Services, obtained through the Freedom of Information Act, found that Health Care Service Corporation, a Blue Cross Blue Shield insurer, had hired EviCore to review prior authorizations. EviCore, the audit found, played a role in making “inappropriate denials” for 30 patients because it failed to keep its cancer guidelines up to date. As a result, EviCore retrained its staff. HCSC did not respond for comment.
Former employees have also questioned how the guidelines were put to use.
A maternal-fetal medicine physician in Colorado, Gail Miller, took a job as a doctor at EviCore in 2018. The idea of ensuring safe medical practices appealed to her. But she soon grew convinced that EviCore was more interested in saving money.
EviCore rejected her suggestions for improving its maternal fetal health guidelines. Her supervisor required her to decide at least 15 cases an hour — or one every four minutes. She often reviewed requests by physicians outside her specialty.
Nine months after starting at EviCore, Miller quit, disappointed by the attitudes of some of her colleagues. “Most of the physicians who work at these places just don’t care,” she said. “Any empathy they had is gone.”
EviCore noted its clinical staff had “high engagement, satisfaction and retention rates.” It said the most common reason for denying a prior authorization is because doctors neglect to include necessary information.
Results
EviCore meets regularly with insurers and state Medicaid programs. It is a critical part of the business. The company has to demonstrate savings or clients will have little reason to continue their contracts.
Typical was a 2019 meeting with Vermont’s Medicaid program, which for years had used EviCore to review coverage requests for advanced radiology and cardiology scans. A slide show demonstrated how the company had helped lower costs for cardiac imaging through denials. Rates had zigzagged, from a high of almost 15% of requests in one three-month period to a low of 6.1% in another.
But the presentation, obtained through Vermont’s Public Records Act, revealed another way that EviCore saved money for insurers. Prior authorization requests for radiology imaging services had dropped to 3,629, a decline of 16%. Cardiology requests had plummeted even more — down 38% in a little more than a year. Doctors had simply stopped asking for procedures for their patients.
An EviCore executive called this the “sentinel effect” at a legislative hearing in Kansas. It is like the sheriff coming to town. Once doctors know EviCore is watching, they make fewer inappropriate prior authorization requests, he said.
Doctors, however, say that such decreases reflect how difficult it is to fight EviCore and similar companies. Their entrance into the market frustrates doctors from making otherwise legitimate requests.
In its statement, Cigna described the sentinel effect differently. The company said that it helps doctors stay up to date on best practices. “Sentinel effect refers to the reduction in frequency with which physicians order inappropriate services because they are now aware of the latest clinical evidence,” the statement read.
A spokesperson for Vermont’s Medicaid program said the state does not believe that EviCore made unfair or unsound coverage recommendations. Instead, EviCore helped Vermont make “sound decisions from both a fiscal and patient care perspective.”
“It is never a goal for the state of Vermont or our third-party contractors to deny service,” said Alex McCracken, spokesperson of Department of Vermont Health Access. “We are committed to delivery of service for our customers.”
Vermont eventually ended its contract with EviCore because it decided to no longer require prior authorization for advanced imaging scans in its Medicaid program.
‘Too much say’
The day after his stress test, Cupp drove to his granddaughter’s high school to drop off her archery bow — it had been left behind in the morning rush. He and his wife went shopping at the grocery store. That evening, he watched as his grandkids showed off some baby frogs they had purchased at a pet store.
He went to bed at 8:30 p.m. in order to wake at 2:30 a.m. for the hourlong drive to his job as a maintenance worker at a medical supplies warehouse just south of Columbus.
At about 10:30 p.m., Cupp’s wife, Vivian, shook Chris awake. “Your dad’s breathing funny,” she told her. Chris ran into their bedroom. Her father was gasping for air. Suddenly, he stopped. Chris began CPR. She told her mom to call 911.
By the time the ambulance arrived at Adena Regional Medical Center, where he had received his nuclear stress test 36 hours earlier, his body was mottled and cool. He had suffered cardiac arrest. The time of death was 11:39 p.m.

ProPublica asked four cardiology experts to review Cupp’s medical situation. One cardiologist said she would not have recommended a heart catheterization. Given his symptoms, which did not include complaints about chest pain, the best diagnostic tool would have been the stress test, she said.
Three others said the heart catheterization was appropriate. One cardiologist noted that Cupp was diabetic, overweight and showed signs of having suffered a prior heart attack. “It’s very reasonable to say we’ll just go straight to a heart catheterization,” the cardiologist said.
If Cupp had received the procedure when first ordered, his life may have been saved, one expert said. “The doctor was absolutely right to order the catheterization. It was certainly necessary,” said Jonni Cooper, president of American Board of Cardiovascular Medicine and a board certified cardiovascular nurse practitioner.

State and federal regulators rarely impose onerous penalties on companies like EviCore.
Connecticut’s Insurance Department recently reviewed EviCore and Carelon. It found no problems with Carelon. EviCore was fined $16,000 this year for more than 77 violations found in a review of 196 files. EviCore is also accredited by two trade associations, which review companies periodically for compliance with industry standards.
Holding the companies legally responsible for their decisions is also difficult. In 2022, Carelon settled a lawsuit for $13 million that alleged the company, then called AIM, had used a variety of techniques to avoid approving coverage requests. Among them: The company set its fax machines to receive only 5 to 10 pages. When doctors faxed prior authorization requests longer than the limit, company representatives would deny them for failing to have enough documentation. Carelon denied the allegations in court and admitted no fault. A spokesperson declined to comment on the lawsuit.
Elevance, Carelon’s parent company, said its subsidiary “is focused on improving health outcomes while also lowering the cost of care.”
This year, Chris, representing Cupp’s estate, sued United Healthcare, EviCore, the Adena Regional Medical Center and Cupp’s doctor, accusing them of malpractice, among other allegations. Cupp’s attorney, John Markus, later decided to drop United and EviCore. Lawsuits against employer-funded health plans, like the one Cupp had with United, must be tried in federal court, where case law favors insurance companies. For instance, insurers found at fault do not pay punitive damages, only the cost of treatment. The medical center and the doctor declined to comment, citing the ongoing litigation. In court, both denied any wrongdoing. United and EviCore declined to discuss Cupp’s case, despite an offer from Chris to sign a waiver of medical privacy rights.
Her father’s death wracked Chris. He had been her best friend. He helped raise her three kids. He provided for the family. Two years before his death, he purchased a new double-wide trailer to replace a rusting single-wide the family had lived in for years. It had four bedrooms, enough for everyone. It stood on the side of a hill, surrounded by oak and maple, a leafy retreat with a view of the valley below.
Cupp was buried at a cemetery across from a cornfield on March 9. A gray granite headstone marks his date of death.
Chris Cupp drives a school bus to make ends meet. For extra pay, she picks up a lot of the trips for night games. She says she hopes that no one else has to go through what she did.
“Insurance has too much say over something that can save your life,” she said. “When it comes to your heart, something that’s going to kill you, they have too much say in that. That’s my thought about it.”
Agnel Philip contributed reporting.
Best Practices for Implementing a New EHR System
Join Seppo Rinne, MD, PhD, as he explores practical strategies for navigating the complex process of transitioning to a new electronic health record (EHR) system. Drawing on real-world experiences from organizations that have successfully implemented EHR changes, learn how to manage the challenges of EHR transitions to enhance workflow efficiency and improve patient care. From initial preparation to system optimization, this session will provide actionable steps for health care administrators, informaticists, clinical leaders, and frontline clinicians and include a live Q&A moderated by Jill Jin, MD, MPH.
Learn more and register here.
Register Now! Medicaid Managed Care Fireside Chat.
Medicaid Managed Care Fireside Chat
Thursday, November 21
12:00 p.m. - 1:00 p.m.
Please join this month's Fireside Chat on November 21, hosted by Dr. Janelle White, Chief Medical Officer of Medicaid, Medicaid colleagues and CEOs from Standard Plans and Tailored Plans.
Topics will include:
- Hurricane Helene response and recovery efforts
- Results from the 2023 Consumer Assessment of Healthcare Providers and Systems
- Medical Clinical Policy Updates
- Pharmacy Updates
- Collaborative Care Capacity Building Program (CoCM)
- Community Alternatives Program (CAP) Referral Process for Children and Disabled Adults

Downed Trees Prompt Wildfire Concerns in Western NC
Trees were strewn about like sticks across western North Carolina after Hurricane Helene brought torrential water currents rushing through valleys.
Now those same washed-out trees and brush are causing concern for wildfires.
The North Carolina Forest Service said this weekend that the potential for increased wildfire activity is above normal in November.
“In the aftermath of [Helene], the amount of fuel on the ground is excessive. Smaller diameter fuels and leaf litter will quickly dry out,” the Forest Service wrote on Facebook.
In addition to the fallen debris providing numerous kindling opportunities, the forest service says they’ll have trouble responding to fires if they break out.
“Damage to roads, unstable, and downed trees will continue to challenge response, making it difficult for first responders to access some wildfires, which increases the potential for large wildfires in the most heavily impacted areas,” the forest service wrote.
Channel 9′s Dave Faherty spoke with a forester with the NCFS who said there’s still a lot of work to be done after Helene.
“We’re expecting people to do more burning this fall. We are worried about access with landowner roads and small woods roads that landowners say they have not had the time to clean out yet,” said Eve Ciotti with the NC Forest Service. ”So if a wildfire does occur we are worried about getting to that fire.”
The forest service says November is one of their busiest months. Last year they had 2,000 wildfires across the state, and 1,200 of them were in the month of November.
But despite the risk, there’s still the need to burn safely. Gary Miller and his son were working to clear trees on their property near Colletsville, but there are so many that they’ll have to cut them up and burn them sometime in the next month.
“We’re going to burn,” Miller told Faherty. “We have to get a burning permit, do everything like we’re supposed to, so we don’t endanger anyone else’s property.”
They say they’re waiting for some rain before setting fire to the fallen trees. Since the storm hit more than five weeks ago, there has been very little rain here.
Some parts of western North Carolina are currently in early drought stages. The NCFS said it’s important to keep an eye on the weather. The agency reminded residents to not burn anything on dry and windy days.
You can find more tips to prevent wildfires at this link. [source]
NC Clinician and Physician Retention and Well-being Consortium LEAD Highlights!
![]()
At the recent LEAD Conference, the North Carolina Clinician and Physician Retention and Well-being (NCCPRW) Consortium reaffirmed its dedication to improving the professional well-being of healthcare workers across the state. Earlier this year, NCCPRW joined forces with the Dr. Lorna Breen Heroes’ Foundation (DLBHF) to launch the ALL IN: Caring for North Carolina’s Caregivers initiative.
On Saturday, DLBHF CEO Corey Feist, JD, MBA and CMO Stefanie Simmons, MD, FACEP addressed conference attendees to share progress on Phase 1 of ALL IN: C4NCC and preview Phases 2 & 3 of the initiative. Phase 1, which began in April, called on hospitals and health systems to remove invasive and stigmatizing mental health language from credentialing applications, addendums, and peer review forms.
Since April, five North Carolina Health Systems, representing 45 hospitals and benefiting 14,000 credentialed health workers, along with the NC Department of Insurance, have audited, changed, and verified that their credentialing applications are free from intrusive and stigmatizing questions regarding mental health conditions and treatment.
We recognize the following recipients as Wellbeing First Champions:
- HCA Healthcare
- Novant Health
- Sentara Health
- UNC Health
- WakeMed Health & Hospitals
- NC Department of Insurance
- revised its Uniform Credentialing Application, enabling many hospitals across the state that use this form to benefit from the change and further update their own supplemental forms.


In the latter part of the NCCPRW Consortium session, Dr. Stefanie Simmons led a panel discussion titled “Leading Sustainable Systems-Change for a Healthy Workforce.” Panelists included Dr. Christina Bowen, Chief Wellbeing Officer at ECU Health; Dr. Nadia Charguia, Executive Medical Director of the Wellbeing Program at UNC Health and Medical School; and Dr. Jeffrey Hatcher, Chair of Physician Professionalism at Cone Health. They shared evidence-informed strategies being used within their organizations to drive and accelerate structural reforms, along with practical advice on initiating changes when resources and budgets are limited.

Be sure to continue checking Morning Rounds, as we share more photos and details from a weekend of recognition and celebration!

Congratulations to the NCMS Member Candidates!

Four NCMS Members Claim Victory in 2024 Election
Congratulations are in order for four members of the North Carolina Medical Society who emerged victorious in their respective races on Tuesday! Their success marks a significant achievement, highlighting the importance of healthcare professionals in state leadership.
North Carolina’s election results revealed a split decision in some of the state's most high-profile races. Voters selected Republican Donald Trump for President, while electing Democrat Josh Stein as Governor. This dynamic points to North Carolinians' nuanced perspectives on governance at both the state and federal levels.
In the state legislature, Republicans maintained control of the Senate with a supermajority, underscoring their stronghold and potential sway in legislative decision-making. However, the House saw a notable shift, as Republicans lost their veto-proof majority, meaning that bipartisan cooperation may now play a greater role in passing state legislation. These results set the stage for a dynamic political landscape in North Carolina, with opportunities for collaboration as well as new challenges ahead.
Congratulations to:
- Dr. Greg Murphy, US House of Representatives District 3
- Dr. Grant Campbell, NC House of Representatives District 83
- Dr. Timothy Reeder, NC House of Representatives District 9
- Mark Hollo, PA, NC Senate District 44
We also extend our deepest gratitude to all of our dedicated member candidates who put their time, energy, and passion into advancing healthcare priorities across North Carolina. Your hard work and commitment to the wellbeing of our communities have not gone unnoticed.
Thank you for your dedication to improving healthcare for all North Carolinians and for your willingness to serve. Your voices, whether in office or out, continue to move us forward in creating a healthier, more equitable future for our communities.
The NCMS talked with all our member candidates prior to the election. To see more of those interviews click here.

The North Carolina Medical Society is Hiring! Join Our Team!
![]()
The North Carolina Medical Society (NCMS) is looking for talented, driven individuals to help us shape the future of healthcare in North Carolina. We are currently hiring for two key positions: Coordinator, Association Management and Manager, Financial Operations.
Manager, Financial Operations - NCMS Foundation
The Manager, Financial Operations manages day to day financial transactions of the North Carolina Medical Society Foundation (NCMSF) and other affiliated organizations. Processes accounts payable and receivables, reconciles bank statements, performs accounting and audit functions and other financial administration of the Enterprise.
Get a full description of the Manager, Financial Operations - NCMS Foundation position here.
Coordinator, Association Management
The Coordinator, Association Management manages the day-to-day needs of the Association Management department. This department manages and operates 14 component associations. Duties include project coordination, conference and event support, membership recruitment and retention, daily accounting functions, responding to member and prospective member inquiries, and preparation and follow-up activities associated with board and committee meetings.
Get a full description of the Coordinator, Association Management position here.
How to apply:
Send your resume to [email protected].

Hurricane Helene and the Impact on Reproductive Health in Western North Carolina
Since Hurricane Helene struck North Carolina in late September, the full spectrum of reproductive health care in the region has been in precarity, from treatment for high-risk pregnancies to abortion care. Western North Carolina’s only abortion clinic is still closed, and third-trimester, high-risk pregnant patients have been transferred out to hospitals across the state, health care workers told States Newsroom.
Dr. Bhaskari Burra is an Asheville-based OB-GYN who works at the only high-risk obstetrics center in western North Carolina. She’s also a fellow with Physicians for Reproductive Health.
The clinic had to close after the storm and wasn’t able to fully open back up until the middle of October, Burra said: “We’re already in a maternity care desert in this area and that sort of further ostracized people from accessing care on the outpatient side.”
Continue reading here.

Baxter International Restarts IV Fluid Solutions Manufacturing at Largest Plant
Baxter International restarted its highest-throughput intravenous solutions manufacturing line at its hurricane-hit North Cove facility in North Carolina, the company announced Thursday.
At its peak operation, prior to Hurricane Helene, manufacturing line represented approximately 25% of the site’s total production and approximately 50% of the site’s production of one-liter IV solutions, the most commonly used size by hospitals and clinics.
Baxter said initial batches will be manufactured concurrently with ongoing quality activities and will only be released in accordance with applicable regulatory requirements to ensure the quality and safety of the products.
“Recovery progress at our North Cove site continues to be very encouraging. In a matter of weeks, our team has advanced from the depths of Hurricane Helene’s impact to restarting our highest-throughput manufacturing line. This is a pivotal milestone, but more hard work remains as we work to return the plant to full production," José E. Almeida, chair, Baxter International president and chief executive officer said in a statement. "I want to recognize the dedication of our North Cove team as well as the countless Baxter employees globally who have committed themselves to helping contribute to supply continuity amid this unprecedented challenge. I also offer Baxter’s gratitude for the steadfast support of ASPR, FDA, the State of North Carolina and HHS. And we are deeply appreciative of our customers’ patience and partnership as progress continues.”
Continue to the full article here.
Capitol Chronicle: Medicare Payment – 2.8% Cut on the Horizon / Working Toward a Fix
Medicare Payment – 2.8% Cut on the Horizon / Working Toward a Fix
On Friday, November 1st, the Centers for Medicare and Medicaid Services issued its final rule on the Medicare Physician Fee Schedule, which includes a 2.8% cut in Medicare physician payment. The payment reduction is scheduled to take effect January 1, 2025.
News of the potential cut was announced mid-year and the North Carolina Medical Society, along with our medical/specialty society partners, has been advocating since that notice for a fix to the anticipated cut. That work will continue in earnest as we approach year-end.
If the payment cut goes into effect, physicians will be facing a fifth year in a row of declining payments while medical practice costs continue to rise. Our message: This is unsustainable, and practices are at the breaking point as they strive to meet Medicare patients’ needs. Practice viability hangs in the balance and shifting patient mix to offset another payment reduction is not an option for many.
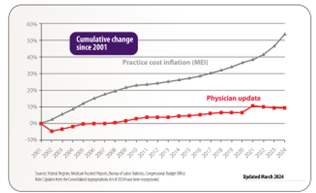
A Fix on the Horizon
Fortunately, our messages are being heard on Capitol Hill and a bipartisan group in the U.S. House of Representatives, led by Rep. Greg Murphy, MD, has introduced legislation to avert the 2.8% cut (H.R. 10073) and to add a positive payment adjustment to help physicians and medical practices absorb next year’s projected 3.6% increase in the medical practice operational cost.
Congress will be headed back to Washington after this week’s election and a fix for Medicare physician payment cut will continue to be our priority during their home-stretch session. Our hope is that a fix won’t be a last-minute rescue as the 2024 clock winds down.
You can help in this effort. Please use this LINK that the AMA posted to send your members of Congress a message stressing another cut in Medicare physician payment is unsustainable. You may have received similar requests from our partner organizations, such as national specialty societies, and we encourage you to use those channels for communicating your concerns as well.
We are also collecting statements and practice profiles from across the state to help in our effort to convey the impact of Medicare payment cuts on practices and access to care for patients. Please email your submissions to be included as examples we can share with our members of Congress.
Thank you. Your engagement matters.
Do you know your state and federal legislators? More importantly, do your legislators know you?
The NCMS can help you connect with policy makers as a constituent and advocate!

