
Register Today for the DOCMS Hybrid Meeting on Prevention of Firearm Injury

REGISTER NOW - Hybrid Meeting
A Zoom link will be sent to all registrants, once the registration closes.
Registration will close on December 13th at 12pm.
“Prevention of Firearm Injury”
DOCMS invites the medical community to learn about firearm policy in NC and to discuss opportunities to intervene and prevent firearm injury in our communities. Moderated by Nancy Henley, MD.
Guest speakers include:
Becky Ceartas is the Executive Director of North Carolinians Against Gun Violence (NCGV) and has been leading the organization since 2014. She has 22 years of experience with non-profit organizations. Becky became involved in gun violence prevention work after the Sandy Hook tragedy. As a new mom, she was compelled to take action. She now works with volunteers and supporters to fulfill NCGV’s mission, which is to make North Carolina safe from gun violence through educating the public about preventing gun violence, enforcing current laws, and enacting needed new laws.
Dr. Brian Eichner is Assistant Professor of Pediatrics at Duke in the Division of General Pediatrics and Adolescent Health and has been at Duke since 2006. Since starting at Duke, he has been interested in the pediatrician's role in preventing gun injury and death and has spoken on this topic in various venues and works with his colleagues on how to discuss firearm injury prevention with families and has worked to improve the provision of gun locks at well child visits across the Duke network. His clinical interests are in the primary care of children with medical complexity and his current research interests are in the early diagnosis of developmental delay and autism.
AGENDA:
6:15pm-6:30pm– Socializing
6:30pm-7:45pm– Dinner, Guest Speakers & Discussion
7:45pm-8:00pm– DOCMS installation of new officers and 2023 schedule
CME Credit is available for this session
Join DOCMS for the last membership meeting of 2022!
University Club
3100 Tower Boulevard, Suite 1700 - Durham, NC 27707
Wednesday, December 14, 2022 | 6:15pm - 8:00pm
A Zoom link will be sent to all registrants, once the registration closes.
Registration will close on December 13th at 12pm.
Questions? Email [email protected]

Register Now for CMS Fourth Quarter Region IV Rural Health Town Hall

CMS is inviting stakeholders to join in it's virtual fourth quarter regional Rural Health Town Hall on Thursday, October 27th.
This is an opportunity to learn and share feedback about CMS programs, resources, and priorities.
CMS encourages stakeholders to submit any topics, questions, or issues in advance to [email protected].
To register for the Town Hall, please click here. Once registered, you will receive a confirmation email with the meeting details.

COVID Variants Gaining Ground Ahead of Expected Winter Surge

While the omicron BA.5 variant cases are beginning to decline, omicron subvariants--BQ.1, BQ.1.1 and BF.7--have gained ground.
Because they appear to have a growth advantage over BA.5, scientists and health officials are closely monitoring these emerging variants.
As we head into winter, health officials are expecting another wave of viral infections. Omicron BA.5 variant remains dominant in the US, making up about 68% of all new infections, down from about 80% at the beginning of October.
Read the full article here.
Wake County Members - Make Your Voice Heard on Community Issues and Activities
![]()
Wake County Medical Society (WCMS) is meeting October 26 at the NCMS Headquarters to discuss upcoming elections, Federal and State Supreme Court cases involving medical practice, and to elect 2023 officers.
Ted Kunstling, MD, WCMS President, urges county members to speak up. "For more than a century, the WCMS has served an important role for us and for our patients."
Kunstling shares a common frustration with some other county societies. "In recent years, these roles have changed, new challenges have emerged, and participation has decreased. Nevertheless, the Society remains a potentially important independent supporter of both our professional and personal lives by maintaining connections. We who have been long-time members, who are “survivors,” recognize the society’s value and seek to preserve it for current and future generations of physicians and surgeons in Wake County." Adds Kunstling, "We need your support and leadership to make this possible. The relevance and the future of the society is in your hands."
*Dinner will be available at 6:30 PM and the meeting will convene at 7:00 PM.
To register or for more information, email [email protected]. To include your County Medical Society news in the Morning Rounds, email Randy Aldridge at [email protected].

Great News for NC Patients: Hearing Aids Now Available Over the Counter

For the first time, hearing aids are available for purchase over the counter at retailers across the United States.
Adults with mild-to-moderate hearing loss can now purchase hearing aids at a store or online without a prescription, medical exam or audiologist fitting--and at savings much more significant than before this historic ruling was issued.
The FDA estimates the new rule could lower average costs for hearing aids by as much as $3,000 per pair, the White House said. Consumers are expected to save about $1,400 per individual hearing aid, or over $2,800 per pair.
Read the full article here.
NCMS Policy Committee Meets In-person for the First Time Since Pandemic

The NCMS Policy Committee met in-person for the first time since the pandemic at NCMS headquarters on October 12, 2022. The Policy Committee is one of two NCMS committees tasked with making policy recommendations to the NCMS Board of Directors.
One of the most important factors considered by the Policy Committee when drafting proposed policies is member feedback, so please be on the lookout for draft policies when they are submitted to NCMS members for feedback! Requests for member comments will be published in Morning Rounds and shared on the NCMS website.
If you are curious about current NCMS policies, please check out the NCMS Policy Manual available here.

Are Colonoscopies Really Effective? New Research Suggests the Value May Be Overestimated

According to new research, colonoscopies may not be as effective at preventing and reducing the risk of colorectal cancer as once believed.
A landmark study suggests the benefits of colonoscopies for cancer screening may be overestimated.
The study is the first of its kind, comparing head-to-head to no cancer screening in a randomized trial, found that colonoscopies reduced people’s risk of developing cancer, but it was far less than what had previously been observed in other studies.
Read the full article here.
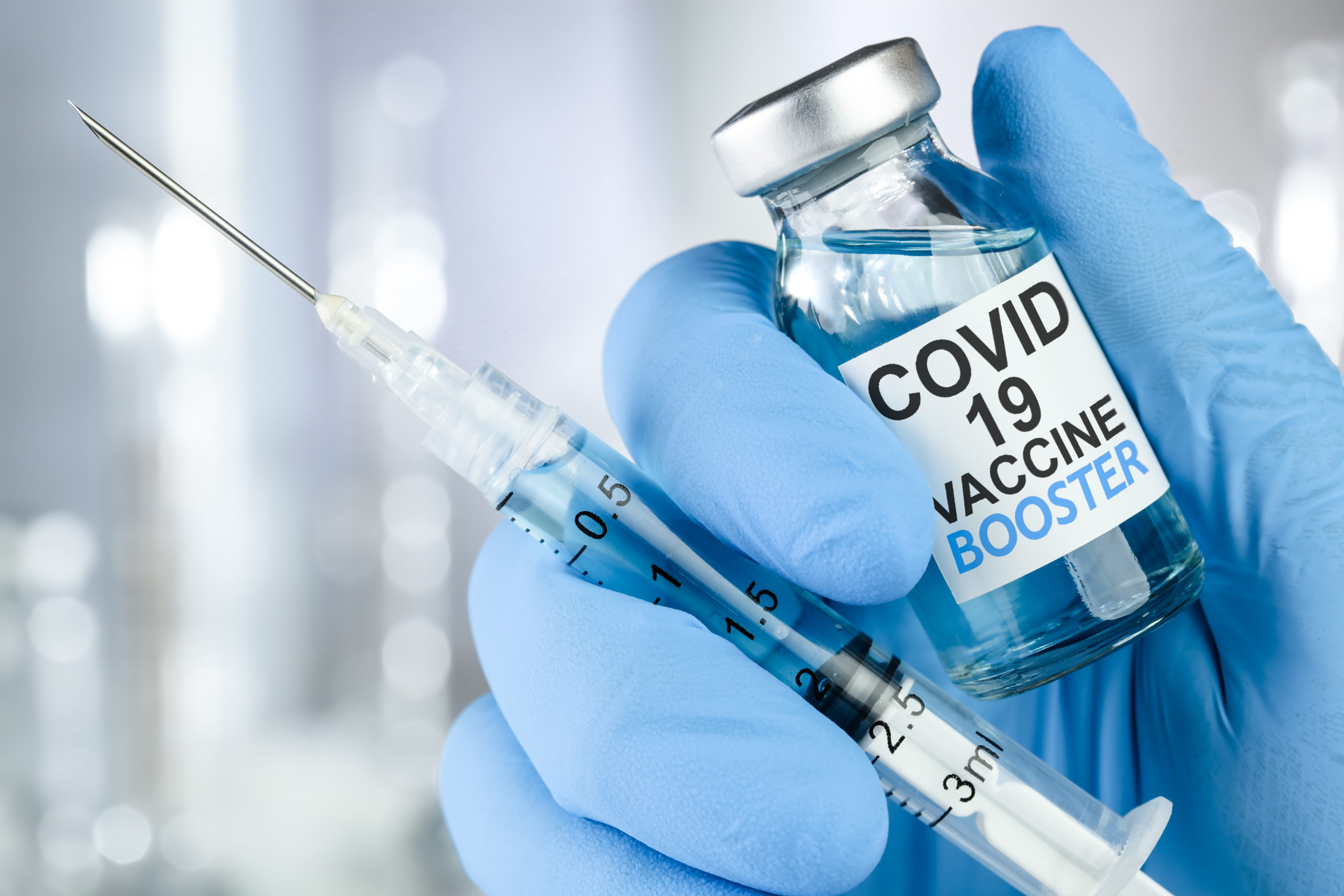
Younger Age Groups in NC Can Now Receive Updated COVID-19 Booster

On Wednesday, the U.S. Food and Drug Administration amended the emergency use authorizations (EUAs) of the Moderna COVID-19 Vaccine, Bivalent and the Pfizer-BioNTech COVID-19 Vaccine, Bivalent to authorize their use as a single booster dose in younger age groups.
This authorization comes ahead of an expected winter wave.
These bivalent COVID-19 vaccines include an mRNA component of the original strain to provide an immune response that is broadly protective against COVID-19 and an mRNA component in common between the omicron variant BA.4 and BA.5 lineages to provide better protection against COVID-19 caused by the omicron variant.
Read the full story here.

Making NC the Healthiest State to Practice Medicine. NCMS Holds First in Series of Meetings

The North Carolina Medical Society hosted the first North Carolina consortium meeting in September to address the systemic issues of clinician burnout and retention.
With a unified goal to make NC the healthiest state for clinicians to practice medicine, a diverse gathering of passionate representatives of medicine has taken place. This is a joint effort from fellow clinicians, mental health professionals, and health care leaders coming together as a team. Development of strategies and innovative support initiatives directed at the improving the resiliency and retention of clinicians.
There is an abundance of optimism and hope within this consortium leveraged by experience and keen insights for change. As this consortium swells in members, so will new opportunities for North Carolina’s medical community. A healthy and supported clinician creates a healthy and supported state.
Learn more about NCMS Wellness and Resilience efforts here.

Masking for NC Health Care Workers Still Recommended

Updated CDC mask guidance eliminates the need for some providers in health care facilities to continue to wear masks; however, NC clinicians are urged to continue masking.
The updated guidance recommendations are based on community transmission data. Currently, no county in NC is considered a low-transmission area.
Learn more about NC's levels here.
CCH Updates Its 2022 Provider Manual
![]()
Carolina Complete Health has updated their Provider Manual to reflect revisions to Utilization Management Guidelines, Tobacco-Free Policy Information, changes to Value-Added Services, and more!
To access the latest version, click here.

Check Your Inbox! NCMS Election E-mails Arriving Now. Deadline to Vote is October 13

You should have received an e-mail from NCMS by now. It is coming from our third party vender, Intelliscan. If you have not seen it, please check your spam folder.
The North Carolina Medical Society Nominating and Leadership Development Committee has issued the final slate of candidates. Under the NCMS’ governance structure, online voting for the candidates will begin on September 29, 2022 and continue until midnight on October 13, 2022.
Paper ballots will be available to those who need them. If you do not receive your ballot, please contact NCMS.
Individuals interested in voting in the NCMS Election must be an active NCMS Member (2022 dues paid).
The following slate of nominees was selected by the Nominating and Leadership Development Committee:
NCMS Board of Directors:

President-Elect: Eileen Raynor, MD
Region 2 Representative: Charul Haugan, MD

At-Large: Merritt Seshul, MD
NC American Medical Association Delegation:

Delegate: E. Rebecca Hayes, MD

Delegate: Karen Smith, MD

Delegate: Roy Syracuse, MD
The following are the members of the NCMS Nominating and Leadership Development Committee:
Chair Phil Brown, Jr., MD
President-Elect Arthur Apolinario, MD
Ex-Officio Michael Utecht, MD
Board Representative Jugta Kahai, MD
Board Representative Eileen Raynor, MD
Region 1 Representative Latonya Beatty, MD
Region 1 Representative Chris Grubb, MD
Region 1 Representative Joe Navejar, DO
Region 2 Representative Justin Hurie, MD
Region 2 Representative Ronnie Laney, MD
Region 2 Representative Madji Namde, MD
Region 3 Representative Labron Chambers, MD
Region 3 Representative Peter Fenn, PA-C
Region 3 Representative Jim Hill, PA-C
Region 4 Representative Tracy Bell, PA-C
Region 4 Representative Frank Melvin, MD
Region 4 Representative MaryShell Zaffino, MD
NCMS Celebrates National PA Week!
National Physician Assistant Week starts today!
The American Association of Physician Assistants was established in 1968 (now known as the American Academy of Physician Assistants) and was instrumental in the development of nationwide standards and PA certification. The American Academy of Physician Assistants) is incorporated in North Carolina.
In 1967, Duke University's Medical Center graduated the first class of Physician Assistants in the country. The program was started to alleviate shortages of primary care doctors. In 1988, Duke University awarded the first Master's Degree for Physician Assistant education.
The NCMS salutes our many PA members who are helping North Carolinians improve their quality of life!
Read more about National Physician Assistant Week here.

Is Your Practice Making These Top 5 Coding Mistakes?

A Medical Economics article highlights the top 5 coding mistakes you could be making, causing your practice to lose revenue. Are you working at your most efficient level?
Read the full article here.
Could A Russian Bat Virus Spark NC's Next Health Crisis?
In 2020, a team of Russian Scientists identified a troubling new virus in horseshoe bats, Khosta-2.
The virus, which share commonalities with SARS-CoV-2, concerned the scientists because of its ability to infect human cells [in lab conditions].
More recently, a separate team of scientists from Washington State and Tulane Universities ran their own tests on Khosta-2, its capability to infect humans and antibody response. They found the initial results concerning. Should you be worried now?
Read the full article here.
NC Clinical Trial Explores Next-Generation Technology

A multicenter clinical trial has found that a device known as a bionic pancreas was more effective at maintaining blood glucose levels than standard-of-care management among people with type 1 diabetes.
The 13-week trial tracked 326 participants, ages 6 to 79 years, who had type 1 diabetes and had been using insulin for at least one year.
The UNC Chapel Hill conducted trial was primarily funded by the National Institute of Diabetes and Digestive and Kidney Diseases.
Read full article here.

NC Breast Cancer Awareness Month Events Happening Around the State

5k Walk - Breast Cancer Research
Sat, Oct 8, 7:00 AM
Cancel Cancer Cornhole Tournament
Sun, Oct 23, 11:00 AM
POUND for PINK - Make Noise for Breast Cancer Support
Sat, Oct 22, 9:30 AM
Pedal In Pink
Sat, Oct 29, 9:00 AM
Ribbons of Hope Social with WSC
Wed, Oct 12, 6:30 PM
Go Pink Network Luncheon
Fri, Oct 21, 11:00 AM
Carvin' for a Cure
Wed, Oct 19, 6:00 PM
Don't Miss Your Chance to Win Bling! Let's Cheers to That!
Joining us at the NCMS Golden Stethoscope Awards Gala? Enter the Bubbles and Bling Raffle to benefit the NCMS Foundation!
Purchase a DELICIOUS flute of Westgate Wines champagne for $25 and be entered to win a FABULOUS piece of JEWELRY from Reeds Jewelers!
Proceeds benefit the Foundation’s programs that improve access to care, health and wellbeing, and empower physicians and PAs to lead.
Many thanks to the Reeds Jewelers and Westgate Wines for making this raffle possible!

Today is National Child Health Day!

National Child Health Day was first established in 1928, under a Joint Resolution of Congress. It is acknowledged annually on the first Monday in October and recognizes the care and guidance children need to grow strong and healthy.
Here are a few ways for you to encourage your patients to participate:
• Schedule your child’s next routine checkup.
• Ensure vaccinations are up to date.
• Schedule a routine dental checkup.
• Add new healthy activities to your children’s routine.
• Set an example by letting your children catch you in healthy habits.
• Inspect your child’s toys. Are they broken or age-appropriate?
• Share your best tips for helping your children live a healthy lifestyle.
Read more about the day here.

Happy Birthday to these NCMS Members Celebrating in October!

John L. Abernethy, Jr., MD, PhD
Robert M. Adams, IV, MD
Feyisayo A. Adeyina, MD
Kamal S. Ajam, MD
Shannon F. Alejandro, MD
Zulfiqar Ali, MD
Fred H. Allen, Jr., MD
Gilbert R. Alligood, Jr., MD
Peter D. Almirall, MD
Charles M. Almond, MD
George A. Alsina, MD
Theresa C. Amerson, MD
William K. Andersen, MD
J. Robert Anderson, MD
Pooja J. Apte, MD
Sasan S. Araghi, MD
Gerald M. Aronoff, MD
Jean H. Ashburn, MD
Kandis D. Atkins, PA-C
Trevor C. Austin, MD
Aleksandra Avery, MD
Claxton A. Baer, MD, PhD
D. B. Baird, MD
David S. Baker, II, MD
Matthew G. Baker, PA-C
Scott W. Baker, MD
Marquiez D. Ballard, PA-C
Robert M. Barr, MD
David W. Barry, MD
Derrick A. Bass, PA-C
Maura C. Bass, PA
Michael P. Battaglino, MD
Carmen J. V. Beamon, MD, MPH
Stacey B. Bean, MD
Ann Y. Becker, MD
Timothy L. Bell, PA-C, MPH
Ross J. Bellavia, MD
W. Tyson Bennett, MD, FACC, FACP
Jill L. Benson, MD
Thomas W. Benton, MD
Jerry C. Bernstein, MD, FAAP
Gary L. Biesecker, MD, FACS
Sukanto Biswas, MD
Billy G. Black, MD
Charles W. Blount, Jr., MD
James D. Bobbitt, MD
Casey E. Bohl, MD
R. Randal Bollinger, MD, PhD
Jeremy J. Bonkowske, MD
Alexandra H. Boster, DO
Josie B. Bowen, MD, FACEP
W. Scott Bowie, MD
Richard F. Bowling, MD
James F. Bowman, MD
Dale W. Boyd, Jr., MD
James D. Branch, MD
Teresa S. Bratton, MD
Jacob R. Brayboy, MD
Mark E. Brenner, MD
Bradley C. Brenton, MD
Thomas E. Brewington, Jr., MD, JD
Don C. Bright, MD
Mary D. Broga, MD, FAAP
Jennifer A. Brooks, PA-C
Chamaine R. Brooks-Locklear, MD
Delores E. Brown, MD
Elizabeth D. Brown, MD
Ernest H. Brown, Jr., MD
Thomas L. Brown, MD
J. Dale Browne, MD
Meredith H. Browne Perez, PA
Charles W. Bryan, MD
John H. Buck, MD
Manuel E. Bulauitan, MD
Julia A. Bulkeley, MD
Christopher T. Bullers, MD
Eithne T. Burke, MD
Timothy A. Burke, MD
Walter Woodrow Burns, Jr., MD
Craig M. Burnworth, MD
Edwin R. Cadet, MD
Molly S. Calabria, PA
James C. Califf, MD
A. Barry Campbell, MD
C. Bradley Carlson, MD
William C. Carr, MD
Marc R. Carruth, MD
Lawrence S. Carter, Jr., MD
Alden K. Casati, PA-C
Thomas E. Castelloe, MD
Christopher M. Cepeda, MD
J. Kenneth Chance, MD
Kerry E. Chandler, MD
Cynamon K. Chawla, MD
Firas Chazli, MD
C. Frank Chen, MD
Hsiupei Chen, MD
Nirav Chiniwalla, MD
Paul S. Chipley, MD
Matthew J. Chovaz, MD
Tara L. Chronister, MD
Badie T. Clark, III, MD
Chad M. Clark, MD
Olivia M. Clelland, PA-C
Kelly M. Clifford, MD
W. Gerald Cochran, MD
Max W. Cohen, MD
Teddy G. Combs, PA-C
Patrick M. Connor, MD
Anna J. Conterato, MD
Scott L. Cornella, MD
Thomas P. Cornwall, MD
Daniel T. Cotter, MD
Benjamin L. Coulter, MD
Mary L. Courrege, MD
Charles J. Court, MD
Christopher D. Covington, DO
R. Wayne Cox, MD
John T. Crawford, MD
Harry D. Crews, MD
Laddie M. Crisp, Jr., MD
Luis J. Cuervo, MD
Julie A. Czech, MD
Kunal S. Dalal, MD
Christopher T. Daley, MD
Nicole M. D'Andrea, MD, MPH, FACOG
Robert D'Angelo, MD
Walter E. Daniel, MD
David M. Dare, MD
Leroy S. Darkes, MD
Deborah H. Davis, MD
Keith E. Davis, MD, FACC, FACP
Michael E. Davis, MD
Samuel P. Davis, III, MD
Katyucia de Macedo Rodrigues, MD
Thomas W. deBeck, MD
R. Prasad DeGala, MD
Larry C. Dekle, MD
Megan A. DeMariano, MD
John W. Denham, MD
Nilay V. Desai, MD, FACE
Ronald W. Digby, MD
John H. Dilworth, MD
Dobrinka V. Dimitrova Koutleva, MD
Meredith G. Disharoon, DO
Regina Dodis, DO
S. Shripad Dongre, MD
S. Trevor Downs, PA-C
Adam N. Drechsler, MD
John E. Drew, MD
Logan S. D'Souza, MD
Julie D. Dunaway, PA-C
Todd H. Duncan, MD
Andrea M. DuPont, MD, FACEP
Suzanne E. Dvergsten, MD
Robert R. Earnest, MD, FAAP
Jason C. Eck, DO
John Stewart G. Edmunds, MD
Bradley S. Ellison, MD
Scott C. Elston, MD
Ravenne A. Eschette, MD
C. Allan Eure, MD
J. Holt Evans, MD
James C. Fahl, MD
William S. Farabow, MD
David E. K. Feldman, MD
Nathan P. Fergus, MD
Ashley M. Ferguson, MD
Michael O. Ferguson, MD
Nicholas R. Fiacco, MD
Lynne C. Fiscus, MD, MPH
Robert R. Fish, MD
Jessica M. Fisher, MD
Thomas F. Flaherty, MD, MPH
T. Sledge Floyd, Jr., MD
James E. Fogartie, Jr., MD
Philip B. Fontenot, MD
Clayton J. Foret, MD
Robert M. Foster, MD
Arnold R. Frazier, MD
Barry I. Freedman, MD
Preston H. Gada, MD
Omar A. Gafur, MD
Louis A. Gagliano, MD
James C. Gaither, MD
Paul G. Galentine, III, MD
Jeffrey Michael B. Galvin, MD
W. Ray Gammon, MD
Lisa M. Gangarosa, MD
Ronald L. Garber, MD
Gilbert J. Garcia, Jr., MD
Brian P. Garvin, MD
Christopher P. Garwacki, MD
R. Glenn Gaston, MD
Paige L. Gausmann, MD
Laura C. Gay, MD
Robert M. Gay, MD
Alfred E. Geissele, MD
Richard W. Geldmeier, MD
Ryan D. Gentry, MD
Gregory R. Gibbons, MD
David E. Gibson, MD
Thomas V. Giguiere, MD
M.G.F. Gilliland, MD
Carrie G. Gill-Murdoch, MD
Charles J. Girard, II, MD
Meredith O. Godwin, MD
Kathryn R. Gordon-Escobar, PA-C
Mark C. Grieb, MD
Soledad C. Griffin, MD
James G. Groce, MD
Stephanie A. Grotzke, MD
Carmelo Gullotto, MD
Anna B. Gulyn, MD
Sandeepkumar J. Gupta, MD
Regina E. Gurley, PA
Bhavna K. Gvalani, PA-C
William D. Hage, MD
Matthew S. Hale, PA-C
Warner L. Hall, Jr., MD
Frank T. Hannah, MD
Kathleen W. Harknett, MD
David K. Harper, MD
Wayne L. Harper, MD
Charles W. Harris, MD
James M. Harris, MD
Jason R. Harris, MD
Anastasia Hastie, PA-C
Chester C. Haworth, Jr., MD
William C. Hayes, Jr., MD
Hubert B. Haywood, III, MD, FACP, FIDSA
Michael N. Heacock, MD
Paul J. Healy, MD
James R. Hedgepeth, MD, FAAP
Edward A. Hedrick, MPAS, PA-C
Jeanette H. Hemp, MD
Shane D. Hemphill, MD
Thomas F. Henley, MD
Georgia A. Hennessy, MD
W. D. Henrichs, MD
John M. Herion, MD
Darrell E. Hester, MD
David A. Hester, MD
Frederick A. Hewett, II, MD, FAAP
Caitlin M. Higgins, MD
Michael D. Hightower, MD
Andrew U. Hines, MD
David E. Hipp, MD
Micaela M. Hofer, PA-C
Byron J. Hoffman, Jr., MD, MACP
Colleen M. Holden, PA-C
Jennifer L. Holmes, MD
Dimitrios P. Hondros, MD
John D. Howell, Jr., PA
Russell M. Howerton, MD
Jeffrey A. Huang, MD
Charles E. Huggins, PA-C, MMS
Christopher L. Hunt, MD
Syed H. Hussaini, MD
Awawu E. Igbinadolor, MD
Russell A. Incatasciato, DO
William F. Ingram, III, MD
Mohammad O. Iqbal, MD
George V. Irons, Jr., MD, FACC
Arin L. Isenstein, MD
Harold N. Jacklin, MD
William A. Jarrett, MD, FACS
Katie R. Jimison, PA-C
Jana G. Johnson, MD
Kenneth L. Johnson, MD
Robin T. Johnson, PA
Curtis B. Johnsrude, MD
Colin D. Jones, MD
Drew A. Jones, MD
Jeffrey D. Jones, MD
John R. Jones, MD
Venkata R. Jonnalagadda, MD, FAPA
Robert C. Jordan, Jr., MD
Ryan M. Jordan, DO
Damilola O. Joseph, MD
Donald G. Joyce, MD
Carmin M. Kalorin, MD
Mukesh N. Kamdar, MD
Robert E. Kanich, MD
William S. Kaufman, MD
Catherine M. Kelly, MD
Todd L. Kelly, MD
Ashton S. Kennedy, PA-C
Brian H. Keogh, Jr., MD
Harold B. Kernodle, Jr., MD
Larry S. Kilby, MD
Mary J. Kirby, MD
Sidney E. Kirkley, MD
Joseph W. Kittinger, III, MD
Michelle E. Klawiter-Benton, MD
George Klein, MD
Aaron D. Kline, MD
Michael W. Klinkner, MD
Autumn Konz, PA
Henryk M. Kowalski, MD
Michal Kozanek, MD
William L. Kozel, MD
Ernest N. Kraybill, MD
Ted R. Kunstling, MD, FCCP
Richard W. Kurzmann, MD
Jeffrey T. Kuwahara, MD
Anthony J. Kwon, MD
Kimberly Kylstra, MD
Jeffrey A. Lamphere, PA-C
Charley W. Lane, PA-C
John G. Langhenry, IV, MD
Michael R. Lawless, MD
Tae J. Lee, MD
Yates A. Lennon, MD, FACOG
Baxter C. J. Leonard, MD, FAAFP
William F. Lestini, MD
Stuart J. Levin, MD
Peter M. Levitin, MD
Caroline M. Lewis, DO
Timothy E. Lietz, MD, FACEP
David M. Lingle, MD
Mark D. Lins, MD
James C. Little, Jr., MD
Timothy W. Longbine, MD
Gandhari Loomis, DO
Robert R. Lopez, MD
James M. Love, MD
Kent V. Lucas, MD
Stephen D. Lucey, MD
Elisa T. Lund, MD
John B. Lykes, MD
Joshua C. Macomber, MD, FACC
Kenneth R. Madsen, MD
Robert P. Majors, Jr., MD
Heidi C. M. Mangelsdorf, MD
Jayadev Manikkam Umakanthan, MD
James T. Mann, III, MD
James R. Manning, III, MD
Gregory A. Mantooth, MD, FACS
Edgar S. Marks, MD
Sheila F. Marshall, DO
Charles T. Marston, Jr., MD
Richard W. Martin, MD
John L. Masonis, MD
Clinton E. Massey, MD
David C. Matthews, MD
John Matzko, MD
Richard J. Max, MD
Kathy D. Mayo, MD
James A. McAlister, Jr., MD
Greig V. McAvoy, MD
Joseph G. McCabe, DO
Patrick S. McElgunn, MD, MBA
James S. McFadden, MD
Douglas S. McFarlane, MD
Jacquelyn A. McGill, MD
Murphy F. McGirt, Jr., MD
Patricia L. McHale, MD
John W. McKay, MD
Netasha S. McLawhorn, MD
William W. McLendon, MD
Michele H. McMillan, MD, FAAP
S. Dean McPhail, MD
Paul J. Meis, MD
Joseph W. Melamed, MD
Morton Meltzer, MD
Mindy L. N. Merritt, MD
Terry M. Messer, MD
Pradeep Mettu, MD
Kai Miao, MD
Adam R. Militana, MD
Emily M. Miller, MD
Philip R. Miller, MD
Chadwick M. Mills, MD
Leanne F. Minnick, PA-C
Anita M. Molby, DO
Richard E. Moon, MD
Robert B. Moore, MD
B. Dawn Moose, MD
Greta S. Morcos, PA-C
Lauren W. Morris, PA-C
Leon M. Morrison, MD
Ashley M. Mortenson, MD
Robert G. Moser, MD
Michael P. Moulton, MD
Kristen M. Mundy, PA-C
Martin J. Murphy, MD
Jason A. Mutch, MD
Francis A. Neelon, MD
Marc H. Nesi, MD
Dale A. Newton, MD
Gunjan Nigam, MD
Ainslee E. Noreen, PA-C
Sean P. O'Brien, MD
Imelda N. Odibo, MD, FACOG
John M. Ogle, Jr., MD
Kenneth G. Olsen, MD
Brian M. Opalacz, DO
Florin M. Orza, MD
Suzette R. Oxendine, PA-C, MMS
John A. Paar, MD
Joshua J. Pagano, DO
Aurora K. Pajeau, MD, MPH
Gaurang M. Palikh, MD, FAAN
Jeffress G. Palmer, MD
Robert M. Palmer, MD
Laurie S. Panzer, PA-C
Amrita Parikh-DeSai, MD
Bill J. Parker, MD
David W. Parker, II, DDS, MD
R. Lamar Parker, Jr., MD
Jerome P. Parnell, II, MD
Marshal R. Parsons, MD
Jacek J. Paszkowiak, MD
Janish J. Patel, MD
Jignasa J. Patel, MD
Praneil Patel, MD
Priyesh A. Patel, MD
Sachin B. Patel, MD
Shilpesh P. Patel, MD
Susanj S. Patel, MD
Jerry E. Patterson, MD
C. Charese Pelham, MD
Prabhakar D. Pendse, MD
Philip S. Perdue, Jr., MD
Jeffrey B. Perrin, MD
Lenin J. Peters, MD
John L. Peterson, MD
Louis W. Pettygrove, PA-C
Edward M. Pickens, MD
Eduardo A. Piqueras, MD
Eric W. Pittman, MD
Jeffrey Pokorny, MD
Matej Polomsky, MD
Henry A. Pool, MD
William L. Porfilio, MD
Charles R. Port, DO
Thomas L. Presson, Jr., MD
Ronald A. Preston, MD
Gregory M. Price, MD
Douglas C. Privette, MD
Ronald J. Prucha, Jr., MD
Richard W. Puschinsky, MD
Meghan K. Pyle, MD
Katharine A. Pyron, MD
Shawn P. Quillin, MD
Aamer A. Qureshi, MD
Abu-Ahmed Z. Rahman, MD, FACP
Michael G. Rallis, MD
Ralph S. Ramos, MD
E. Allison Ramsey, MD
Tom S. Rand, MD
Stewart F. Rasmussen, MD
Janakiram Ravulapati, MD
Patrick M. Reames, MD
Michael A. Reardon, MD
Marshall S. Redding, MD
Monica B. Reddy, MD
Tyce L. Regan, MD
Robert L. Reid, MD
David A. Rendleman, III, MD
Rodolfo C. Reyes, MD
James M. Rhyne, MD
Claudia W. Richardson, MD, MPH
John C. Rickabaugh, MD
Miriam E. Ridley, MD
Waldemar L. Riefkohl, MD
Craig A. Rineer, MD
George E. Rinker, MD
Janet L. Rippel, PA-C
April M. Risinger, PA-C
John G. Roach, III, MD
Karen Y. Robinson, MD, FAAP
George D. Robison, IV, MD
Ryan C. Romano, DO
Sara L. Rooker, MD
Brandon S. Rorie, PA-C
J. Lawrence Rouse, III, MD
Brandon P. Roy, MD
Ranjan S. Roy, MD, PhD
Michael R. Ruffolo, MD
Jeffrey W. Runge, MD, FACEP
Timothy E. Ryan, MD
Jill A. Rys, PA-C
Samy R. Saad, MD
Frank Sabiston, Jr., MD
Scott A. Sample, DO
Richard Sanchez, MD
Jos R. Santz, I, MD
Thomas R. Saullo, MD
Charles D. Scheil, MD
John L. Scheitler, MD
Irvin G. Scherer, MD
Neil E. Scheurich, MD
Michael H. Schlesinger, MD
Jessica N. Schloesser, DO
Jeffrey S. Schmidt, MD
Jennifer L. Schnering, PA-C
Andrew M. Schulman, MD
Steven J. Schwam, MD
Lindsey K. Seaver, PA-C
Paul B. Segebarth, MD
Monica A. Selak, MD
Andrew T. Selfe, PA-C
Jeffrey F. Severa, DO
Charnette H. Shade, MD
Disha N. Shah, DO
Rickin A. Shah, MD
Nasfat Shehadeh, MD
Pheston G. Shelton, IV, MD
John D. Shepherd, MD
Sufia Siddique, MD
Adeel M. Siddiqui, MD
C. Van Sikes, III, MD
William J. Simons, MD
Jason F. Simpson, MD
Ronald W. Singer, MD
Puneet P. Singh, MD
Jay A. Singleton, DO
Anthony F. Skalak, MD
Scott C. Sledge, MD
Anne B. Smith, MD
Ellison L. Smith, MD
Hannah C. Smith, PA-C
Karen L. Smith, MD, FAAFP
Whitman E. Smith, Jr., MD
William T. Smith, MD
Douglas J. Snyder, MD
Clinton R. Soriano, MD
Mark O. Speight, MD
Michael A. Spencer, MD
Joel F. Spragins, MD
Robert K. Stack, MD
Michael D. Stadiem, MD
John A. Stahl, MD
J. Andrea Staneata, MD
John H. Stanley, Jr., MD
Rodney J. Stanley, MD
Edwin A. Stevens, MD
Ryan W. Story, MD
Elizabeth A. Stratton, PA-C
Christian J. Streck, MD
Helena G. Summers, MD
Brian A. Sumner, MD
Sever C. Surdulescu, MD
Gregory M. Swank, MD, FACS
Brooks W. Taber, MD
Khurram B. Tariq, MD
David E. Tart, MD
David T. Tayloe, III, MD, FAAP
Blucher E. Taylor, MD
Jonathan H. Taylor, MD, FACS
Richard L. Taylor, MD
Trevor M. Taylor, MD
S. Eldora Haworth Terrell, MD
T. Eugene Terrell, MD
Andrew M. Terzian, MD
Debra J. Tetreault, MD
Zsuzsanna P. Therien, MD
Dimitri M. Thomas, MD
Henry C. Thomason, Jr., MD
Aaron B. Thompson, MD
Allie Y. Thompson, PA-C
Lindsey N. Thornton, DO
Thomas G. Thurston, III, MD
Sabah S. Toma, MD
James L. Toussaint, MD
Charles E. Trado, MD
Henry W. Traylor, Jr., MD
James M. Tsahakis, MD
Alex Y. C. Tse, MD
Matthew K. Tsuei, MD, FACS
Mary Catherine Turner, MD, FACP, FAAP
Pamela A. Turpin, PA-C
Marili Uno Witt, MD
Elizabeth C. H. Upton, MD
Daniel S. Uri, MD
Michael J. Utecht, MD, FACEP
Fred H. Van Nynatten, MD
Mark D. Van Poppel, MD
John H. Vance, MD
Carlos A. Vargas, MD
Shona S. P. Varghese, MD
Bradley K. Vaughn, MD
Reid C. Vegeler, MD
Kinga M. Vereczkey, MD
Ananda L. Vieages, MD
John D. Vrnak, PA-C
Phuong-Mai J. T. Vu, MD
Gwendolyn F. Wagoner, MD
Scott D. Wait, MD
Phillip J. Walker, MD
Donald K. Wallace, MD
Russell E. Warburton, MD
Thomas L. Warren, MD
Ronald P. Waterer, MD
Jerry L. Watson, MD
Seth F. Weaver, II, MD
Dakota R. Webster, PA
Rebecca Y. Weinshilboum, DO
Michael S. Weizman, MD
Briana H. Welch-Denton, PA
Brittany L. West, PA-C
Mark J. Whalen, MD
Anthony H. Wheeler, MD
James H. Whicker, MD
Thomas H. White, MD
Russell R. Wilford, Jr., MD
Carey C. Williams, MD
Daniel M. Williams, MD
Emily C. Williamson, MD
Warren L. Williamson, MD
Larry F. Willis, MD
Paul A. Willman, DO
Brett L. Wilson, MD
Lisa K. Wilson, MD
Robert B. Wilson, II, MD
Christopher A. Winter, MD
S. Lamont Wooten, MD
David O. Wright, MD
Stefanie N. Xenakis, PA
Makram A. Yassa, MD
Pavan K. Yerramsetty, MD
Ming Yin, MD, PhD
Andrew S. T. Yoon, PA-C
Thomas A. Zban, MD
Stuart B. Zeilender, MD
Stephanie V. Zeller, MD
Matthew L. Zettl, MD
Bradley J. Zins, MD
Jason D. Zook, MD
David A. Zvara, MD

NC Organization Envisions Equal Health Equity For All

Digging deeper into the data--with a focus on ethnicity and race--the North Carolina Association of Free & Charitable Clinics discovered a startling trend. White patients fared better than patients of color, a common outcome throughout the health care system.
The association, which provides health care services to uninsured and underserved residents, believed it was already making great strides in promoting health equity in a state with one of the largest uninsured populations, but the data painted a different picture.
Armed with a goal to improve what this troubling data showed, a new initiative was implemented by the association, Our Journey Toward Health Equity, which brought together a 29-member Health Equity Task Force composed of association staff, board members and clinic leaders for intentional discussions about health equity.
The North Carolina Association of Free & Charitable Clinics hopes to improve health outcomes for historically marginalized racial and ethnic groups.
Read full article here.

Are You Crossing the Line With Your Patients?
When questioned about doctor-patient friendships, nearly 30 percent of respondents to a survey say they do indeed make friends with their patients.
Respondents who avoided these friendships cited concerns about objectivity as one of the key deterrents to such relationships.
Over-familiarity with a patient can lead to assumptions about a medical condition. A patient who is a friend may shy away from sharing certain medical details, leading to both under and overtreatment.
The American Medical Association (AMA) Code of Medical Ethics: Patient-physician Relationships stops short of addressing friendships.
Read the full article here.

Can A New Tool Help NC Doctors Predict Mortality Risk for Patients With Dementia?

More than 6 million Americans are living with Alzheimer's, a type of dementia that affects memory, thinking and behavior. By 2050, this number is projected to rise to nearly 13 million.
In 2020, 180,000 North Carolinians were living with the disease. By 2025, this number is expected to increase by 16.7%.
A prognosis prediction model may help clinicians accurately predict death among older adults with dementia.
Research published in JAMA Internal Medicine suggests the tool, which measures age, sex, body mass index (BMI), and physical fitness, may help clinicians better frame discussions about treatment and end-of-life decisions with patients.
Red the full article here.

NCMS Members: Are You Feeling Burned Out?

Physician burn out is a growing cause for concern. It is happening across the country and here in North Carolina. Christina Maslach, PhD, a social psychologist and researcher at the University of California Berkeley identified six factors that influence burnout:
- Work overload
- Lack of control
- Insufficient rewards
- Breakdown of community
- Sense of unfairness
- Conflicting values
In a recent episode of AMA Update, Dr. Paul DeChant, a healthcare consultant and co-author of Preventing Physician Burnout: Curing the Chaos and Returning Joy to the Practice of Medicine, discusses these factors driving physicians' high burnout rates.
View the video here.

NC Medical Board Chief Medical Officer Karen Burke-Haynes, MD Invites You to the NCMS LEAD Conference and Gala
Mark your calendar for the NCMS LEAD Conference, Golden Stethoscope Awards, and Presidential Inauguration Gala. The fun starts Friday, October 14th in Raleigh! For full details, click here.

New Report Shows Startling Number of Young Physicians Would Not Choose Medicine Again. Why?

According to Medscape's 2022 Young Physician Compensation report, only 68% of young physicians would choose medicine again.
13,064 physicians in 29 specialties were polled between Oct. 5, 2021 and Jan. 19, 2022.
Young physicians cited dealing with difficult patients (22 percent), long work hours (19 percent) and having so many rules and regulations (18 percent) as their top three challenges as the most challenging part of their job.
Read the full article here.

Don't Miss these Upcoming NC Medicaid Managed Care Webinars

The North Carolina Department of Health and Human Services Division of Health Benefits and North Carolina AHEC are offering an evening webinar series to help providers, practice managers, and quality managers succeed with Medicaid Managed Care.
Sessions are designed to deliver late-breaking information and guidance on NC Medicaid’s transition to Managed Care.
These webinars are hosted by Shannon Dowler, MD, Chief Medical Officer of the NC Division of Health Benefits, and take place the 3rd Thursday of the month from 5:30-6:45 PM.
Upcoming Webinars:
October 20, 2022
November 17, 2022
December 15, 2022
Register for Hot Topics webinars here.
Missed a webinar? Access the NC Medicaid Managed Care Hot Topics Webinar Series Archives here.

Doctors Urge More Research Into Little-known STI Linked to Infertility

Doctors are urging more research into a little-known sexually transmitted infection that has been linked to infertility and miscarriage.
Mycoplasma genitalium, or M. genitalium or M. gen is a sexually-transmitted bacterial infection that may cause genital pain, bleeding and swelling.
M. genitalium has developed resistance to the most common antibiotics used to treat STIs, which is prompting urgency for more research and testing.
Similar to chlamydia and gonorrhea, M. gen. is sometimes asymptomatic, but it may lead to severe complications in both men and women. In men it can cause urethritis, a swelling and irritation of the urethra. In women, M. gen. is associated with cervical swelling, pelvic inflammatory disease, miscarriage, preterm birth, and infertility.
Read the full article here.

NCMS Alliance Virtual Discussion: Diabetes Education in the Latino Community

Please join the North Carolina Medical Society Alliance for a Member Connect virtual gathering on diabetes education in the Latino community with Angela Lamb, DNP, FNP-BC.
When: Wednesday, September 28 at 12:00 noon
Where: via Zoom call (Zoom Link)

Angela Lamb, DNP, FNP-BC, clinical assistant professor in the UNC Charlotte School of Nursing, will speak about her doctoral research with Latino Type 2 diabetes patients in the clinic setting.
Type 2 diabetes disproportionally affects members of the Latino community in the U.S. Dr. Lamb works at the Camino Clinic in Charlotte, one of the member clinics of the North Carolina Association of Free and Charitable Clinics. Her work designing and implementing culturally focused diabetes education classes has led to better disease management among the community she serves.
We hope you will join to learn more about this health challenge facing fellow North Carolinians and some of the work being done to improve health outcomes.

NCMS CEO Chip Baggett Invites You to Attend North Carolina's Most Anticipated Fall Event!
Make Plans to Join Us October 15th in Raleigh for the Golden Stethoscope Awards and Presidential Inauguration Gala! You're not going to want to miss this amazing event!
For full details, click here.
Take a minute and fill out the NCMGMA Salary & Benefits Survey

The North Carolina Medical Group Managers Association (NCMGMA) has opened its salary and benefits survey and are asking practices to complete it between now and November 23rd.
The survey results provide comparative information and highlight industry trends that are useful for practices and organizations in determining critical business decisions.
Participants who complete the survey (minimum of 75%) will have access to the results once they are released in December.
For more information about the survey or to start the survey, please click here.

New Duke Study: Can Artificial Intelligence Detect Autism?

The Duke Center for Autism and Brain Development has been awarded a $12 million federal grant from the National Institute of Child Health and Human Development to develop artificial intelligence tools for detecting autism during infancy and identifying brain-based biomarkers of autism.
In a project, artificial intelligence will automatically code video footage of young children’s behavior and interactions with their caregivers from a digital app used by parents at home. Information collected is used to identify behavioral characteristics of infants and toddlers who are later diagnosed with autism.
A second project will use artificial intelligence to analyze 260,000 health insurance claims, including those from 6,000 children diagnosed with autism, from birth to 18 months.
That data will be used to develop an algorithm to predict autism during infancy and identify the nature of early medical conditions associated with a later diagnosis of autism.
Read the full article here.
NCMS Foundation Webinar: Treating Hepatitis C in Patients with Substance Use Disorders
Register now for the webinar: "Treating Hepatitis C in Patients with Substance Use Disorders"
Rick Moore, MD, AAHIVS
Assistant Professor, UNC Family Medicine
NCDHHS Viral Hepatitis Medical Director
Monday, November 14, 2022
12:00 PM to 1:00 PM
We would like to invite you to a webinar, focusing on optimizing treatment of Hepatitis C in patients with active or recent substance use. It will focus on treatment strategies, examination of available data about safety and efficacy of treatment, and local and state initiatives to maximize care.
What: Treating Hepatitis C in Patients with Substance Use Disorders Webinar
When: November 14th from 12:00 pm - 1:00 pm
Who: Physicians, advanced practice providers, nurses, and healthcare staff involved in the care of people with substance use disorders.
Why: The aim of this webinar is to discuss rationale behind and strategies for achieving broader uptake of Hepatitis C treatment for patients with active or recent substance use. New Hepatitis C infections are highest in young adults, with the majority of these infections being tied to injection drug use. Available data in real world and study settings has demonstrated that treatment of Hepatitis C is safe and effective, and expansion of treatment in this setting stands to have a dramatic impact on individual and public health.
This webinar is free but you must be registered to attend.
Space is limited so register early!
After you register, you will receive an emailed confirmation with webinar and phone-in instructions.

Rick Moore, MD, AAHIVS
About Dr. Moore:
Richard (Rick) Moore II, MD, AAHIVS, obtained his medical degree from Virginia Commonwealth University. He then attended family medicine residency training at the Lawrence Family Medicine Residency in Massachusetts, where he underwent an integrated training track in care of patients with HIV and Hepatitis C. He worked for Rural Health Group from 2014-2019, a federally qualified health center in northeastern North Carolina, where he directed their HIV, viral hepatitis, and medication-assisted treatment programs and served as associate medical director. He continues to provide HIV and Hepatitis C care in this setting and to direct those programs. He helped develop the Carolina Hepatitis Academic Mentorship Program, which trains North Carolina providers in low-resource settings in Hepatitis C care delivery. He serves as the medical director for the North Carolina Department of Health and Human Services Viral Hepatitis Program, a role which he began in November 2020. He is an assistant professor for the University of North Carolina’s Department of Family Medicine in Chapel Hill, a role which he began in July 2019.
Register here.

HCA Healthcare opens North Carolina Hospital

FRANKLIN, NC -- Nashville-based HCA Healthcare has opened a $68 million hospital in Franklin, N.C.
Angel Medical Center is part of HCA's Mission Health, which is based in Asheville, N.C.
The center is a critical access hospital, has a 30-bed inpatient unit capacity, three operating rooms, an endoscopy suite, and a 17-bed emergency department. Outpatient services include a wound clinic, a full laboratory, digital mammography, CT, MRI, nuclear medicine, and physical, occupational, and speech therapy.
Learn more about Angel Medical Center here.

In Memoriam: Marian Wahba Ghraib, MD
NCMS member Marian Wahba Ghraib, MD, died Wednesday, September 7. She was 35 years old.
Dr. Ghraib was affiliated with the UNC Medical Center, North Carolina, where she served the Rocky Mount community.
She attained her medical degree from Case Western Reserve University in Cleveland, Ohio, in 2015 and completed her residency in otolaryngology at Temple University, in Philadelphia, Pennsylvania.
Dr. Ghraib was a research fellow at the National Institutes of Health from 2009 to 2011, after graduating from the University of California, Berkeley in 2019 with a degree in Cell and Molecular Biology.
The staff and members of the North Carolina Medical Society extend our deepest condolences to her family and loved ones.
Read Dr. Ghraib's complete full obituary here.

NCMS Partners With Radio One on Annual "Take A Loved One to the Doctor Day"

The NCMS has partnered with Radio One affiliate stations to sponsor the annual "Take a Loved One to the Doctor Day."
The annual event was started in 2001 and is held every third Tuesday in September.
Today Radio One's affiliate stations in the triangle area -- WQOK 97.5, WFXC 107.1 and 104.3, and WNNL 103.9 -- are promoting routine health screenings and annual physical examinations among African Americans and other ethnic minority groups who have disproportionately high rates of chronic health conditions.
Listen all day to hear appeals by your fellow NCMS members.

The 2022 Golden Stethoscope Award Winners ARE...

Rebecca Hayes, MD, MBA-HM, CPE, FAAFP
Dr. Rebecca Hayes is the first 2022 Golden Stethoscope Award winner!
After more than two years of sacrifice and hard work it is time to celebrate again! The North Carolina Medical Society is honoring physicians and PAs who went above and beyond during the COVID-19 pandemic. Each day this week we are announcing the winners. YOU can join them at the Golden Stethoscope Awards Gala on October 15.
About Dr. Hayes:
Rebecca Hayes, MD, MBA-HM, CPE, FAAFP currently serves as the Vice-Chair of Clinical and Community Operations in the Department of Family Medicine and the Assistant Specialty Medical Director of the community clinics in the Emerging Care Model Division at Atrium Health. She leads the primary care community and teaching clinics in the Greater Charlotte Area through positive healthcare delivery transformation to better care for and improve the lives of underserved communities, while also developing highly skilled, competent, and compassionate primary care physicians. In her 15 years with Atrium Health, Dr. Hayes has served as medical director and core faculty at Elizabeth Family Medicine, and associate program director for Cabarrus Family Medicine Residency Program. In addition she is currently a Clinical Associate Professor in the Department of Family and Community Medicine at Wake Forest University School of Medicine. She was selected as the 2009 Cabarrus Family Medicine Residency Family Physician of the year. Prior to joining Atrium Health, Dr. Hayes had the honor to serve in multiple leadership positions within the US Navy Medical Corp to include faculty and team leader at Naval Hospital Pensacola Family Medicine Residency Program, Senior Medical Officer for the Naval Aviation Technical Training Center Medical Clinic, and Regimental Surgeon, 10th Marines, 2nd Marine Division, Camp Lejeune, NC. Dr. Hayes holds a Bachelor of Arts in Chemistry from UNC-Greensboro and is a graduate of the Medical University of South Carolina College of Medicine. She completed her family medicine residency at Naval Hospital Bremerton, WA and her Faculty Development Fellowship at the University of North Carolina at Chapel Hill. Dr. Hayes earned her MBA in Healthcare Management from Western Governor’s University in 2021. Dr. Hayes lives in Concord, NC with her husband and 8 year old son. They enjoy all things Disney/Star Wars and spending time at the beach.
More winners will be announced all week!
It is time to leave the lab coat at the office and dust off your dancing shoes! Join Dr. Hayes and all your NCMS colleagues on October 15 at the 2022 Golden Stethoscope Awards Gala.
Tickets are going fast. Click here to get yours!

Will New Offer From Hospitals Jolt Stalled NC Medicaid Expansion Negotiations?

The NC Healthcare Association has delivered a proposal to the General Assembly and the Governor that calls on the General Assembly to quickly pass Medicaid Expansion.
In the proposal put forth Friday, health systems and hospitals would fund much of the state’s share of the expense of expanding Medicaid for 600,000 North Carolinians. The proposal also suggests that the state repeal CON law for psychiatric inpatient beds and chemical dependency beds.
North Carolina remains one of only a dozen states that has not expanded Medicaid.
Read the full article here.

Picture Perfect! NCMS Photo Contest Results Are In and They're Spectacular
Congratulations to the 2022 NCMS Photo Contest Winner

“Nature’s Beauty, Big and Small”
The beautiful image above, taken by first-time Photo Contest participant Brian Bowman, MD, PhD, is the overall winner of our member photo contest this year. His photo, “Nature’s Beauty, Big and Small,” will grace the cover of our NCMS 2023 calendar. Congratulations, Dr. Bowman!
This year over 50 photographers participated in the contest.
Kudos to the winners in the other categories!
Nature Category Winner: Karl S. Chiang, MD – “Mystic Swamps”

North Carolina Category: Charles H. Classen, Jr., MD – “The End of the Small Family Farm North Carolina”

Travel Category: Kathryn McConnell Greven, MD – “Yucca at Dawn”

Wildlife Category: Joel B. Miller, MD – “GRUBHUB Delivery”

FINALISTS:
Brian Bowman, MD, PhD "Nature's Beauty, Big and Small"
Karl S. Chiang, MD "Mystic Swamps"
Charles H. Classen, Jr., MD "The End of the Small Family Farm North Carolina"
Kathryn M. Greven, MD "Yucca at Dawn"
Joel B. Miller, MD "GRUBHUB Delivery"
Matt Atkins, MD "Slot Canyon"
T. James Baden, MD, FACP "Canadian Tranquility"
P. Mark Gallerani, MD "Atlantic Puffins"
Steven M. Genkins, MD ("Seadoc") "The Restless Sea"
Marion McCrary, MD, FACP "Clarity of Reflection"
Thomas J. Monaco, Jr., MD "Autumn Cascades"
Arnold C. Olegario, MD "Let's Keep It Green"
Danna Park, MD, FAAP, FACP "Currituck Lighthouse Spiral"
Leighton A. Raynor, MD "High Jump"
SEMI-FINALISTS:
Yun L. Boylston, MD, MBA "A Walk in the Woods"
Jeffrey Coston, DO "Looking Glass Falls"
M.E. Dossenbach, PA-C "Monarch Butterfly Feeding on Milkweed"
Jane Girskis, PA-C "Crazy Tree Root"
John Goldfield, PA-C "Coastal Fife Trail, St. Andrew, Scotland"
Jim Hill, MEd, PA-C Emeritus, DFAAPA "Red Shoulder Hawk in Rain"
H. Slade Howell, MD "Flying Squirrel with New Home"
Rodger Israel, MD "Yates Mill in Autumn"
Andrew S. Lamb, MD "Assisi, Italy at Sunset"
H. Curtiss Merrick, MD, FACP "Baby Owls with Sweaters"
David Mertz, MD "Vallarta Surprise"
Vikas Patel, MD "Trees Mimicking Barn Color"
Katherine J. Pierce, MD "One Moment in Time"
Heather Pol "Kiawah in June"
Demetri T. Poulis, MD, FACS "Sunset, Nags Head, NC"
HONORABLE MENTIONS:
Herbert W. Clegg, II, MD "Bear Cub Up a Tree"
Lisa M. Gangarosa, MD "Fall Creek Gorge in June"
Lawrence Greenblatt, MD, FACP "An Unusual Visitor in Urban Durham"
Richard M. Griffin, MD "Kayaker"
Hampton A. Howell, MD "The Lee Side"
Anna Malysz Oyola, DO "Violet Dawn"
Donna M. Richardson, MD, MBA "Rainy Day"
James A. Salisbury, MD "The Get Away"
Nadine B. Skinner, MD, FAAFP "Clowning Around"
David Tart, MD "Isle of Iona, Scotland Beach"
David Thomas Tayloe, Jr., MD, FAAP "Sunset at Hawkins Landing"
Robert E. Taylor, MD "Sunset at Ocean Isle Beach"
John G. Wagnitz, MD "Writing Spider"
Michael R. Wolff, MD "Southport Yacht Basin"

Congratulations, Columbus Regional! Now the region's first Center for Excellence in Robotic Surgery

Congratulations are in order for Columbus Regional Healthcare System. It has achieved accreditation from Surgical Review Corporation (SRC), becoming the region’s first Center of Excellence in Robotic Surgery.
This accreditation recognizes Columbus Regional’s commitment and high standard of delivery of quality patient care and safety.
Columbus Regional has been performing and perfecting robotic surgeries since 2011.
Read full article here.
NC Doctors: Could Your Practice Benefit from the Collaborative Care Model?
The North Carolina Department of Health and Human Services, Division of Health Benefits (DHB) has partnered with NC AHEC to provide educational and practice-based support to primary care practices interested in implementing the Collaborative Care Model.
Collaborative Care Model (CoCM) is an integrated modality that provides patients with medical and behavioral health care in a primary care setting.
The Collaborative Care Model leverages a team-based, interdisciplinary and systematic approach to screen, diagnose, treat, and provide follow-up care.
A Primary Care Provider (PCP) leads the Collaborative Care team, which includes a Behavioral Health Care Manager (BHCM), Psychiatric Consultants, and other mental health professionals acting as force multipliers of behavioral health expertise.
Learn more about CoCM here.

Earn CME credits and ABFM Activity Points While Enjoying the Beautiful Grove Park Inn this December!

The North Carolina Academy of Family Physicians (NCAFP) is delighted to welcome you to the 2022 Winter Family Physicians Weekend, December 1 – December 4, 2022, at the Omni Grove Park Inn in Asheville, NC!
The weekend's timely and requested general session topics, complimentary CME workshops, and innovative satellite seminars mean approximately 25+ AAFP Prescribed Credits are up for grabs.
Learn more and register for the event here.
Junkie. Drunk. Addict. Words Matter When Talking to Patients About Substance Use Disorder.
Junkie. Drunk. User. Habit. Dirty. Clean. Addict. User. Alcoholic.
Words, and how you use them when talking to patients, can have a profound effect on people. Talking about addiction in ways that are stigmatizing—meaning words are used that portray someone with a substance use disorder (SUD) in a shameful or negative way—may actually prevent them from seeking treatment.
While addiction is a treatable disease, many people make it more difficult with the language they use. The good news is that simple changes can reduce and eliminate the harmful stigma surrounding substance use disorder.
NIH’s National Institute on Drug Abuse produced an Addiction Language Guide for Clinicians to help change language and reduce or avoid sigma.
For more information on how you can help your patients, click here.

UNC Med Students Push for Medicaid Expansion

On Wednesday, UNC medical students, backed with a 500-signature petition, called on UNC Medical School to press the state's hospital association to agree to regulator reforms as part of the Medicaid expansion bill.
The UNC students called on their medical school dean to press the association to back off so the Senate bill can move forward.
UNC Medical School students, faculty, staff and alumni signed a letter suggesting that UNC Health consider leaving the association if the association won’t “prioritize Medicaid expansion over financial interests.”
Read the full article here.
ICYMI: CDC Issues Updated Guidance on Bivalent COVID-19 Booster Doses

On September 13, 2022, presenters at CDC’s Clinician Outreach and Communication Activity (COCA) discussed the new guidance on bivalent COVID-19 booster doses for people ages 12 years and older, including those who are moderately or severely immunocompromised.
If you were unable to hear the call, slides and a recording are available and can be viewed here.

NC HealthConnex Deadline Approaching!

The deadline to connect to NC Health Connex, North Carolina's Information Exchange, is Sunday, January 1st, 2023.
All health care providers who receive state funds (Medicaid, NC Health Choice and State Health Plan) for the provision of health care services must connect to NC HealthConnex to continue to receive payments for services provided, with the exception of voluntary provider groups outlined in House Bill 70 (N.C. Session Law 2019-23). In response to the COVID-19 pandemic, the COVID-19 Recovery Act (NCSL 2020-3) extended the deadlines for certain provider groups.
For more information, visit the Health Care Provider FAQs page here.
For general FAQs about NC HealthConnex, click here.
Updated COVID-19 Vaccines at No Cost to Your Patients

The Department of Health & Human Services (HHS), through CMS, announced that people with Medicare, Medicaid, Children’s Health Insurance Program coverage, private insurance coverage, or no health coverage can get COVID-19 vaccines, including the updated Moderna and Pfizer-BioNTech COVID-19 vaccines, at no cost, for as long as the federal government continues purchasing and distributing these COVID-19 vaccines.
Read full news alert here.

Medicaid's Transition to Managed Care: What You Need to Know

The North Carolina Department of Health and Human Services (NC DHHS) Division of Health Benefits and North Carolina AHEC (NC AHEC) are offering an evening webinar series to help providers, practice managers, and quality managers succeed with Medicaid Managed Care.
These informative webinars are hosted by Shannon Dowler, MD, Chief Medical Officer, NC Division of Health Benefits and moderated by Hugh Tilson, Director of the NC AHEC Program and takes place on the 3rd Thursday of the month from 5:30-6:45 PM.
The Medicaid Managed Care Webinar Series is dedicated to bringing you late-breaking information and guidance on NC Medicaid’s transition to Managed Care.
Don't miss these upcoming Managed Care Webinars:
September 15, 2022
October 20, 2022
November 17, 2022
December 15, 2022
For information, click here.
Are You Talking to Your Patients About Prostate Cancer Screening?
September is Prostate Cancer Awareness month.
During Prostate Cancer Awareness Month, talk to your patients about their risk and screening options.
About 1 in 8 men will be diagnosed with prostate cancer during his lifetime. Prostate cancer is the most common non-skin cancer diagnosed in men, and the second leading cause of cancer deaths in men.
The American Cancer Society’s estimates for prostate cancer in the United States for 2022 are:
- About 268,490 new cases of prostate cancer
- About 34,500 deaths from prostate cancer
Many insurances, including Medicare, covers prostate cancer screenings.
For more information, visit the CDC Prostate Cancer webpage or National Cancer Institute Prostate Cancer webpage.
Also, check out theses Medicare Resources:
Prostate Cancer (PDF) data snapshot
Get information for your patients: Prostate cancer screenings

Warning: Doctors Should Watch for Signs of EV-D68

Pediatricians and top health officials are warning about an uptick in activity of a common virus that, in rare cases, can cause a polio-like syndrome in young children.
Recently, the Centers for Disease Control and Prevention (CDC) issued a health alert to providers about the enterovirus known as EV-D68.
While this bug is common and typically only causes colds, occasionally, children infected with it will develop limb weakness and a progressive form of paralysis called acute flaccid myelitis, or AFM. Other symptoms include drooping eyelids and trouble swallowing or speaking. Pediatric infectious disease physicians are urging pediatricians and clinicians at emergency departments and urgent care centers, as well as parents, to be on the lookout for early signs of AFM.
The CDC issued the following recommendations for healthcare providers:
- Consider EV-D68 as a possible cause of acute, severe respiratory illness (with or without fever) in children. Adults may also become infected with EV-D68, but it is thought to be more commonly detected in adults with underlying conditions.
- Consider laboratory testing of respiratory specimens for RVs and EVs (typically part of multiplex respiratory assays) when the cause of respiratory infection in severely ill patients is unclear, if not already part of typical diagnostic routine.
- Provide supportive clinical management for RV or EV, including EV-D68. There are no available vaccines or approved antiviral treatments.
- Report clusters of severe respiratory illness to local and state health departments.
- Strongly consider AFM in patients with acute flaccid limb weakness, especially after respiratory illness or fever, and between the months of August and November 2022.
- Collect specimens from multiple sources (cerebrospinal fluid [CSF], serum, stool, and a nasopharyngeal [NP] or oropharyngeal [OP] swab) from patients presenting with possible AFM as early as possible and preferably on the day of onset of limb weakness.
- Coordinate with your state public health laboratory to send AFM specimens to CDC for AFM and polio testing.
- Maintain vigilance and report possible cases of AFM to the state or local health department using the patient summary form.
Read full article here.