
2025 Mid-year Congressional Advocacy Update
A New Year / A New Administration / A New Congress
Following the presidential election every four years, there is typically a period of several months for things to settle in on Capitol Hill. The transition with arriving members of Congress, along with new committee appointments, presidential cabinet hearings and a shuffle in office assignments takes some time, and substantive business usually gets underway before spring arrives. 2025 has seen a delay in that timeline due to the President’s and the new administration’s exertion of authority and influence. Since the first of the year, numerous executive orders have been issued, with considerable impact on multiple branches of government, and the emergence of the Department of Government Efficiency (DOGE) has also been a jolt to the status quo across multiple government agencies. Most notable targets include research funding (NIH) and public health guidelines (HHS).
Issues that were on the short list of federal legislative priorities at the outset of 2025 included:
- Medicare payment fix
- Medicare telehealth coverage
- Prior authorization relief
- Step therapy relief
- Workforce expansion needs
- Research funding preservation
- Physician/clinician wellness
Medicare Physician Payment
2024 wrapped up with an intense push to avert the anticipated 2.8% Medicare physician pay cut scheduled to go into effect on January 1, 2025. The prospect of eliminating the cut was very good until the President’s new Department of Government Efficiency (DOGE) torpedoed the year-end legislative package – known as a Continuing Resolution – which was to be the vehicle for a remedy for Medicare payment.
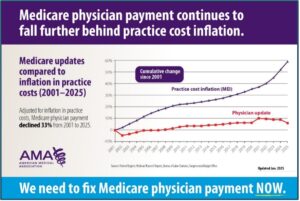
The 2.8% cut ultimately went into effect (“Grinched by Congress) as of the first of the year so the new year brought with it a renewed commitment to reform Medicare physician payment. The 2025 reduction represents the fifth straight year of cuts to physicians, and from 2001 to 2025, physicians have now seen a decline in Medicare payment of 33% when adjusted for inflation (graphic below).
To address the growing Medicare payment dilemma, Congressman Greg Murphy, MD (NC-3), along with a bipartisan group of his House colleagues, introduced new legislation – H.R. 879 / Medicare Patient Access and Practice Stabilization Act to stop the 2.8% cut in Medicare physician payment while also providing a positive payment update to help practices absorb the increasing costs they are facing. Upon introducing the legislation, the goal was to get it incorporated into the Congress’ next funding measure, another Continuing Resolution, that was enacted at the end of March. The NCMS went “all in” to get all 14 of our North Carolina members of the House on the bill as co-sponsors to help its potential for advancing. The Society partnered with a coalition of national and state medical society partners in sending a letter to US Senate and US House leaders emphasizing the urgency of fixing Medicare payment. A March 5, 2025 Alert urged North Carolina physicians to contact their US House members, followed by another Alert on March 9, and we were successful in getting nine N.C. members of the House to formally join the bill. The measure was ultimately not included in the March funding package as hoped, so the House of Medicine redoubled its efforts to keep the Medicare payment reform issue as a foremost priority.
Recent NCMS messaging to Congress has emphasized the impact of Medicare payment cuts in North Carolina, as evidenced by the survey of NCMS members in 2024 Q4 – Results. And, NCMS board member, Dr. Karen Smith, helped strengthen that advocacy effort and message through an op-ed column in her local newspaper, the Fayetteville Observer.
H.R. 1 / One Big Beautiful Bill
In addition to the delays in getting up to “business as usual” speed that resulted from the waves of directives coming out of the White House and new administration, the introduction and controversy around H.R. 1 / One Big Beautiful Bill (OBBB) has been the most time consuming issue on the federal legislative front through the first half of 2025. This legislation was the President’s number one priority at the outset of his term in office. Though the bill drew a lot of attention for its impact on Medicaid and other healthcare-related issues, it was actually a tax funding bill to extend the tax cuts that were enacted in 2017 and due to expire in 2025. To cover the cost of the tax cut extension, Congress was charged with making budget cuts to absorb the cost of the cuts. That directive put Medicaid in the crosshairs along with the Supplemental Nutrition Assistance Program (SNAP) an student loan funds.
At the outset of the discussion of the measure and with several areas of concern emerging, the NCMS sent North Carolina’s members of the US Senate and US House a letter to call attention to how the OBBB would be very consequential for North Carolina. Additionally, the NCMS had multiple meetings with our congressional offices and subsequently sent each of our 14 House members a follow-up letter outlining the various elements of the proposal that would be detrimental to our state. The bill eventually passed the House and the NCMS similarly reached out to our Senate members with a letter of concern as they deliberated over the legislation.
In addition to our Society-initiated advocacy and member communications in May and June, the NCMS also partnered with multiple other stakeholders to help add volume to our messaging. The Society joined multiple sign-on letters that were delivered to Capitol Hill.
Coalition of State Medical Associations letter – February 28, 2025
Coalition of State Medical Associations letter – June 4, 2025
Coalition of State Medical Associations letter – June 24, 2025
As broadly publicized in the media and through NCMS communication, the OBBB passed and was signed into law by the President on July 4, 2025. One bright spot in the enacted legislation is that Medicare physician payment will increase by 2.5% for 2026 – a one-year adjustment. An initial impact assessment from NCDHHS has reported the following.
Work requirements
- Adds a work requirement for Medicaid expansion states (Ages 19–64) – 80 hours per month minimum.
- Exemption: Parents, guardians and caretakers with children 14 or younger.
- Effective: December 31, 2026. (Can appeal for a 2-year extension)
- 250,000 North Carolinians projected by to be impacted.
Provider taxes
- Reduces the current 6% Provider Tax cap down to 3.5%
- Project $ Impact to NC: $22.5 billion over 10 years
- Effective: October 1, 2026.
Healthcare Access and Stabilization Program (HASP)
- HASP payment cuts will begin in 2028
- Impact: $6B
Eligibility / Enrollment
- States will be required to check eligibility every 6 months instead of annually, starting December 31, 2026.
- The change in frequency will result in county social services offices being challenged to double their productivity.
- Delays in eligibility determinations are anticipated.
Medicaid Expansion
- R. 1 will result in increased cost to NC Medicaid due to the work requirement and the lower ceiling for provider tax.
- Work requirements bring new administrative costs.
- Capping provider taxes at 3.5% instead of 6% will add new cost to the state.
- State/federal funding shift expected to activate the “trigger” provision in Medicaid expansion law.
Action Options for the NC General Assembly
- Enact technical correction to the hospital provider tax funding formula to cover the administrative costs needed for work requirements.
- Change the “trigger law” and appropriate state funds.
- Change the “trigger law,” which could result in Medicaid Expansion being discontinued and authorize an alternative financing mechanism.
Mid-Year Re-set
With the OBBB having been enacted and signed into law, attention has shifted back to the legislative issues that had been prioritized at the first of the year . . .
- Medicare payment reform
- Prior authorization relief
- Step therapy relief
- Telehealth flexibilities extension
- Workforce
- Physician/clinician wellness
One additional issue that has emerged recently is inappropriate upcoding by Medicare Advantage plans. As a result, S.1105 / No UPCODE Act was introduced in the Senate to ensure that charges for treatment align with patients’ relevant medical conditions and that Medicare Advantage health plans aren’t able to overstate the severity of their plans’ enrollees’ health condition. A companion bill in the House is anticipated.
North Carolina Physicians Go to The Hill
Multiple groups of physicians have headed to Washington, DC this year to take medicine’s message to Congress. The NCMS has engaged with numerous partner organizations, such as the American Medical Association at their National Advocacy Conference, to advocate for quality patient care and the medical profession.
