

HCA Acquired Mission Hospital in 2019, Dr. Martin Palmeri Speaks Out
(From Barron’s Magazine, June 14, 2024, Catherine Dunn) — When HCA Healthcare inked an agreement to buy the main hospital in Asheville, N.C., late in the summer of 2018, the stock popped 2%. But when nurse Molly Zenker first heard news of the possible sale, her heart sank.
Zenker had worked for HCA once before, at a hospital in Florida, one of the company’s largest markets. She says a stressful experience with bare-bones staffing made her question whether she could remain a nurse. “I was really just trying to put fires out all day,” she says. The picture looked brighter when she switched to a hospital where nurses were unionized, and later when she moved to Asheville in 2017 and found a job she loved at nonprofit Mission Hospital, close to her family. The work felt sustainable and focused on patient care.
Mission, a well-regarded hospital network in the Blue Ridge Mountains, also appealed to HCA. The company completed the deal for $1.5 billion—one of its biggest-ever acquisitions—in February 2019. HCA’s share price has marched upward since, increasing more than 140% in five years and easily outperforming the S&P 500 index
.
Nashville-based HCA is the country’s largest for-profit hospital operator, with 179 hospitals in 19 states. Across its territory, the company has honed a business model that delivers industry-leading profit margins. The stock has benefited as it acquired more hospitals around the country. At the same time, those acquisitions often brought significant staffing reductions at the hospitals, a Barron’s investigation shows.
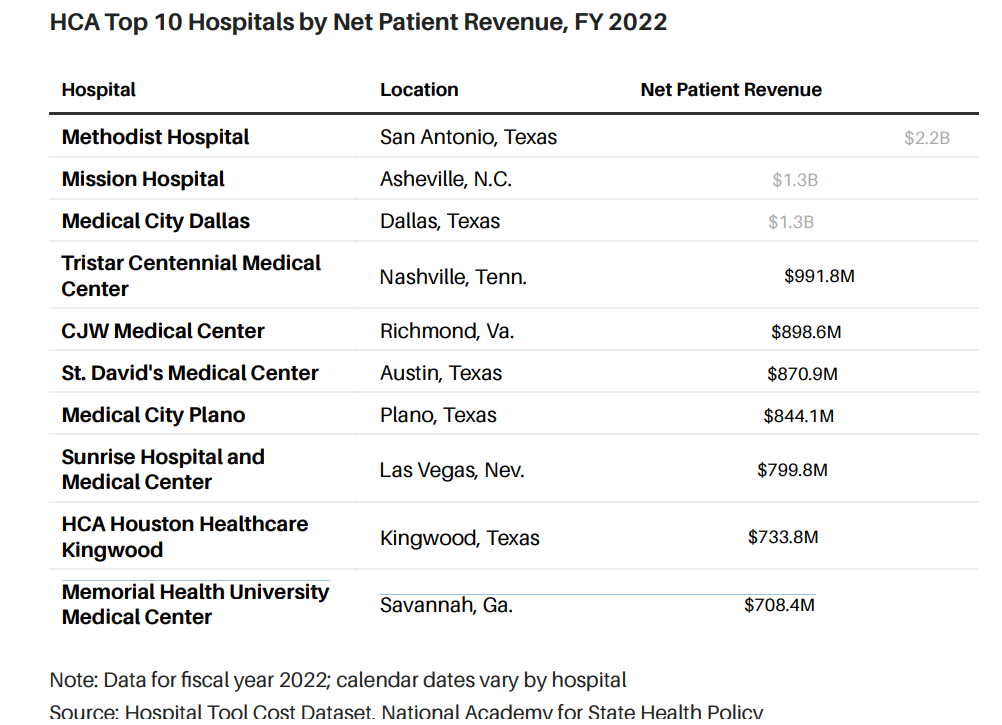
Big Business
HCA owns 179 hospitals across 19 states. Mission, acquired in 2019, is now its second largest hospital by revenue.
At Mission, Zenker and other unionized nurses have publicly decried low staffing and stretched workloads. Dozens of physicians signed an open letter this past fall saying Mission’s quality was suffering under new ownership. The state attorney general filed a lawsuit in North Carolina Superior Court in December, accusing HCA of breaching patient care commitments agreed to during the sale.
The company is fighting the suit. “We are meeting, and in many cases exceeding, our obligations in the purchase agreement,” Harlow Sumerford, HCA’s director of media relations, told Barron’s in an email.
Late last year, inspectors linked four patient deaths to Mission’s failures in their assessment of hospital conditions. The Centers for Medicare and Medicaid Services issued a finding of “immediate jeopardy” that placed Mission’s federal funding at risk.
Regulators have accepted the hospital’s plans to correct problems, and state inspectors, on behalf of Medicare, revisited Mission in May. HCA says the issues have been resolved. “Mission Health continues to be recognized as one of the top hospitals in the country in third-party quality and patient safety ratings, including Health grades, which named Mission Hospital one of America’s 50 Best Hospitals,” Sumerford said.
Mission is the second-largest hospital in the HCA system by net patient revenue, generating nearly $1.3 billion in 2022, according to federal data. It’s one of more than a dozen hospitals that HCA acquired between 2017 and 2021. Barron’s examined 12 HCA acquisitions for which data are available, and found staffing decreased at two-thirds of the hospitals between the year of purchase and 2022.
HCA’s Hospital Acquisitions
Patient care staffing has generally fallen at hospitals following their acquisition by HCA. Here’s a look at 12 hospitals acquired by HCA since 2017 for which staffing data are available.

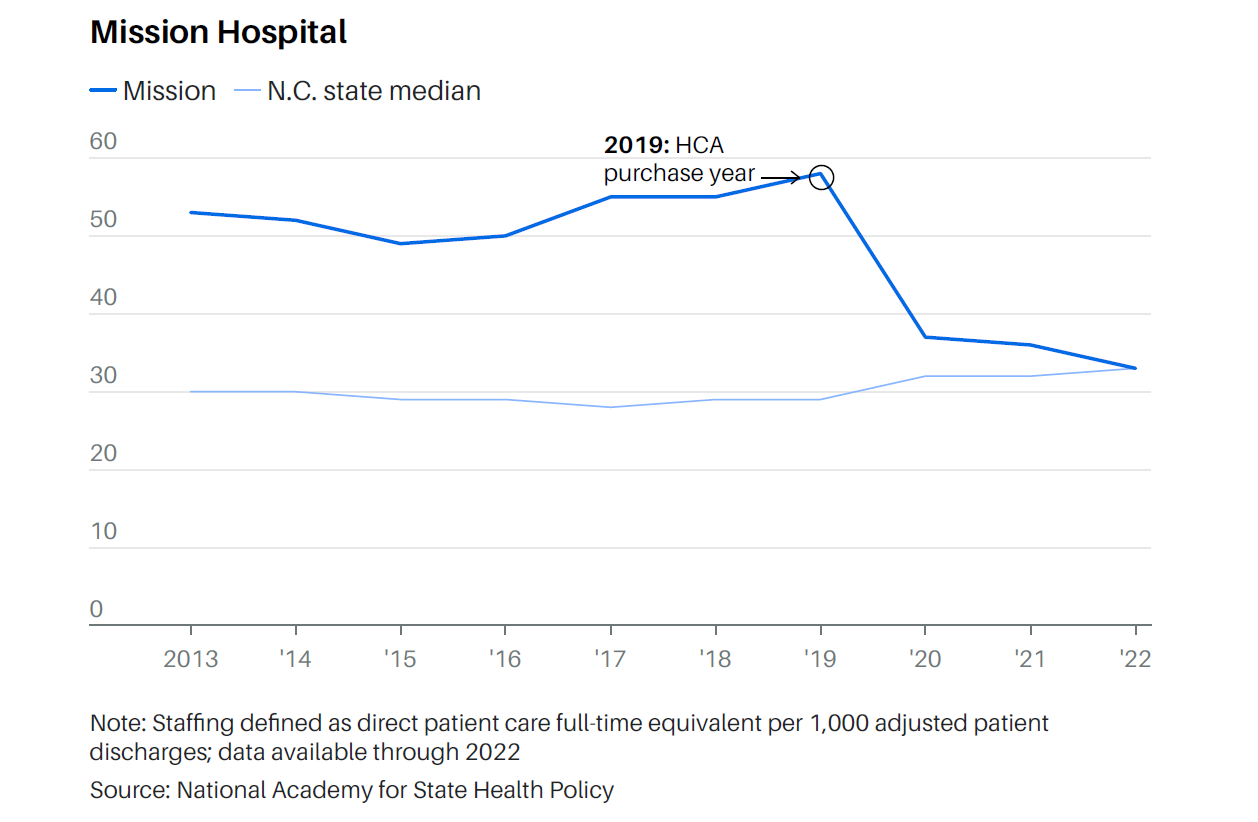
Within two years of HCA’s purchase, direct patient care staffing at Mission fell 36%, according to data from the National Academy for State Health Policy, a nonpartisan think tank. Hospitals that saw other steep staffing declines soon after HCA bought them include facilities in Rochester, N.H. (a 26% drop), Waycross, Ga. (a 22%drop), and Springfield, Tenn. (an 18% drop).
HCA’s staffing decreases contrast with state trends during the same period, according to Barron’s analysis. In New Hampshire and Tennessee, median staffing remained relatively flat, while in Georgia and North Carolina, median patient care staffing rose through 2022,the latest year for which data are available.
Staffing Declines
These four hospitals saw steep reductions in patient care staffing in the years following their acquisition by HCA.
Hospitals are still dealing with the pandemic legacy of staff turnover and higher labor costs—and nurse staffing is at the crux of the matter. Mission nurses are among thousands of unionized nurses across six states now in contract negotiations with 17 HCA hospitals.
While hospitals say there aren’t enough nurses to go around, unions maintain that deteriorating working conditions are keeping nurses away.
There’s little debate about the importance of nurses. Studies show that higher staffing levels are associated with better patient outcomes, including lower mortality rates and fewer injuries from falls during hospital stays. Still, regulations on nurse-to-patient ratios are few. California and Oregon are the only states that require minimum ratios throughout a hospital; just a handful of states set ratios in specific medical units like the ICU.
For this article, Barron’s used a hospital-cost tool managed by the National Academy for State Health Policy. The group pulls in federal Medicare data from hospitals to analyze staffing levels relative to patient volume. Its measure includes labor time for employees and contracted staff involved in patient care, such as physicians, nurses, and pharmacists. Such hospital reporting on staff and contract labor informs Medicare reimbursement rates.
HCA raised several objections to using the data to compare hospital staffing over time, or to other health systems. Sumerford, for instance, noted that Mission Hospital changed how it reported some contract labor in 2022.
“Medicare cost reports are not intended to be used for in-depth staffing analysis, so it is nearly impossible to do an apples to apples comparison between different years or different hospitals,” he said in an email.
“Despite the labor challenges all hospitals are facing, staffing at HCA Healthcare’s hospitals is safe, appropriate, in line with other community hospitals, and in compliance with applicable regulations,”Sumerford told Barron’s.
The company didn’t respond to questions about how it makes personnel decisions and whether it tracks its own hospital staffing levels. NASHP says the Medicare data are vital for policymakers, given that the largest portion of U.S. healthcare spending goes to hospitals.
“NASHP uses Medicare Cost Reports because they are publicly accessible, comprehensive annual reports completed and attested toby hospitals to provide factual cost information to the federal government,” says Maureen Hensley-Quinn, a senior director for the group. “We recognize the complexity across hospitals, but all Medicare Cost Reports are completed based on the same instructions, and data from these reports can offer insights into individual hospitals that are not easily accessible or available otherwise.”
While problems in Asheville have made the spotlight, federal regulators have flagged staffing problems and patient safety concerns at HCA facilities in several other states.
The Georgia hospital that HCA acquired in 2017—Memorial SatillaHealth—came under scrutiny during a 2022 inspection in whichregulators determined the facility “failed to ensure an adequatenumber of nursing staff” to provide care, records show. One nursedescribed staffing levels in the intensive care unit as “truly unsafe”given the demands of monitoring patients on ventilators or IV insulindrips, according to federal records. She told regulators that hercomplaint was “swept under the rug.”
Since 2022, two other HCA hospitals, one in Salem, Va., and one in Panama City, Fla., have also been flagged by Medicare officials for inadequate staffing, according to federal reports.
HCA says the issues at all three hospitals have been resolved.
Maximizing Profits
Tensions over for-profit medicine go back decades. But as the Covid-19 crisis mode recedes, healthcare ownership is attracting new scrutiny, particularly as players like HCA get bigger, while other ventures run into financial trouble. Steward Health Care System, an owner of 30 hospitals, recently filed for bankruptcy protection, a saga closely followed by The Wall Street Journal.
While HCA has produced strong returns for investors— Barron’s recommended the stock in December —a chorus of advocates say the company’s business model isn’t compatible with prioritizing patientcare.
State Sen. Julie Mayfield, a Democrat whose district encompasses Asheville, told Barron’s that her office regularly fields complaints from HCA patients. She’s at the forefront of a community push for improvements at Mission. Their fight has a larger resonance, she says:“ We are the poster child for the corporatization of medicine.”

Kerri Wilson, a nurse at Mission in Asheville, says the work nurses do to keep patients safe doesn’t necessarily translate as billable. “I thinkt hat’s why nursing gets kind of pushed aside,” she says. “It’s not a billable task for us to be able to take you to the bathroom.”
HCA was founded as Hospital Corporation of America in 1968 by investor Jack Massey and doctors Thomas Frist Sr. and Thomas Frist Jr., father and brother to former U.S. Senate Majority Leader William Frist.
HCA has twice gone private, most recently in 2006 through a leveraged buyout led by Bain Capital and KKR, among others. When the company relisted on the New York Stock Exchange in 2011, shares opened at $30 a piece. They now trade around $320.
Stellar Returns
HCA’s stock is up 358% over the past seven years, a period in which the company has expanded its national footprint through multiple acquisitions.

In November, HCA held its first investor day in two decades. During the event on a Nashville stage, CEO Sam Hazen said the company had a “sacred responsibility” to patients, alongside accountability to shareholders: “And we believe that we can harmonize both objectives and accountabilities and ultimately produce value for both.”
The presentations touted the company’s clinical capabilities, including treating strokes, complex heart attacks, and burns. They also told a story of standout financial performance. One analyst in the audience, Kevin Fischbeck at BofA Securities, noted that HCA forecasts margins that are “consistently above what we think about peers being able to generate.”
Indeed, HCA tops industry competitors. Last year, HCA delivered a19.6% Ebitda margin, compared with 17.2% for Tenet Healthcare and 12.2% for Universal Health Services. Ebitda, or earnings before interest, taxes, depreciation, and amortization, is a commonly watched metric to track ongoing cashflows at a business.
Economies of Scale
HCA is the nation’s largest for-profit hospital company. It also has industry-leading profit margins.

On a more traditional accounting basis, HCA also outperforms. Its net income margin, profit divided by revenue, was 8.1% last year, more than double that of Tenet.
At the investor day, company executives highlighted several drivers for HCA’s leading margins: scale that lowers administrative and fixed costs; management systems that help lower costs per patient day; and patient offerings that also enhance returns, whether that’s a specialized cardiac procedure or treatment for burn survivors.
HCA’s hospitals aren’t merely competing against other health systems; they are competing internally against one another. In November, the company showed analysts a systemwide dashboard to track more than 160 key performance indicators at each of its hospitals, which totaled 183 at the time.
Mike Marks, an HCA veteran who recently became the company’s chief financial officer, said that leaders at every one of its hospitals can check these metrics—in areas including labor management, human resources, and physician costs—to identify their hospital’s performance gaps. Marks put it this way during the investor day: “No one really wants to be 183, right?”
The company declined to provide Barron’s with a full list of the indicators used for the dashboard.
Trouble in Asheville
For nearly two decades, Mission Health operated as a state-sanctioned monopoly. A North Carolina law allowed Asheville’s two main hospitals to merge under one nonprofit owner in 1998. Over the years, Mission acquired several rural hospitals, as well. In exchange for this antitrust immunity, Mission was subject to state oversight and limits on margin growth. Then, in 2015, state legislators voted to repeal those supervisory measures. Three years later, HCA stepped in with an offer.
Many in and around Asheville would like to move on from HCA. In Brevard, N.C., home to a small rural hospital that’s part of Mission’s network, local leaders began documenting concerns about staffing levels and physician departures in 2020, a year after the sale.
Mayor Maureen Copelof, a former Navy captain, met with HCA’s chief executive in May 2022 and asked if the city could buy the hospital back; Hazen declined, she says. But the CEO offered to work more closely with the community, according to a letter memorializing the meeting, which Copelof shared with Barron’s. The agreement fell apart, she says, after Brevard sued HCA in a pending case that alleges HCA has abused its market position to charge predatory prices.
HCA has denied allegations of anticompetitive behavior. A federal judge denied the company’s motion to dismiss the suit in February.
Calls for change intensified this past fall, when dozens of doctors throughout the community signed an open letter stating that Mission’s quality of care deteriorated after the HCA acquisition.

“I haven’t seen this degree of physician discontent, community discontent, to my knowledge, in any area of North Carolina,” says Dr. Martin Palmeri, an oncologist at Messino Cancer Centers. In 2019,following HCA’s purchase, he and his colleagues decided not to renew their physician service agreements with Mission and moved to new offices outside the hospital; physicians in the group continued to provide certain treatments at Mission until this past fall.
The practice determined it could no longer treat patients with complex blood cancers at Mission because of safety concerns related to insufficient nursing and pharmacy support.
One of the patients at Palmeri’s practice, Jessica Clements, worries about her healthcare options in the future. She was diagnosed with a type of leukemia in 2021 and initially received good treatment at Mission. But over time, she says she observed nurses in the cancer unit take on increased workloads. Now in remission, Clements fears a relapse because she’d have to drive hours to seek treatment elsewhere.
HCA’s dominance in the Asheville area leaves would-be patients with few choices for care. “If you’re having a heart attack or a stroke or a trauma issue, you have to go to Mission whether you like it or not,” says Karen Sanders, an RN patient advocate in private practice. She recommends that any patient who goes to Mission bring a friend or family member and document the experience.
The findings in the Medicare inspection report—made public in February by the Asheville Watchdog, a local news outlet—were “absolutely shocking,” Sanders says. One critically ill patient, a 48-year-old man diagnosed with bacterial meningitis, went into cardiac arrest after he was left unmonitored and his IV medication ran dry, regulators found.
“The hospital’s leadership failed to ensure a medical provider was responsible for monitoring and ensuring the delivery of care to patients presenting to the emergency department,” the report said.
Molly Zenker left Mission in 2021 after she said a patient fell to the floor because of inadequate staffing. She returned to the hospital last year. She is raising her children in Asheville, she told Barron’s, and she’s committed to making the hospital a better place for her friends and neighbors. ”It needs to be a good hospital,” she says. “That was really what brought me back.”